-the study or a theory of the nature and grounds of knowledge especially with reference to its limits and validity
Two weeks ago I went to dinner and drinks with members of the London ACEs (Adverse Childhood Experiences) Hub, it was a small group in which everyone came from very different backgrounds and professions including some with lived experience. You can see some of us here.
It struck me that the diversity of our group was evidence that expertise in Adverse Childhood Experiences and developmental trauma cannot be held by any specialty. Nobody can claim epistemic dominance. Like the blind men feeling an elephant and each being certain that the whole creature resembles the part they are feeling, in matters of trauma nobody can claim to be able to see the whole picture. Modern medicine is structured with specialists at the top and generalists (like GPs) at the bottom. The Telegraph newspaper has had a series of headlines recently pointing out that GPs don’t know enough about cancer or antidepressants or anything else. According to The Telegraph if people are sick, they ought to a specialist. These are easy accusations to make and have been news headlines for my entire career and will continue until journalists understand and value the fact that generalist knowledge about the ways different illness interact is not the same as the accumulation of number of different specialisms. There were two GPs at the LAH dinner and drinks, evidence perhaps that GPs more than any other specialty see the ways that biography and biology are constantly affecting each other leading to familiar pattens of physical, psychological, and social disruption. Nevertheless, our medical perspective only captures part of the picture which is why our group includes people working in criminal justice, racial justice, education, community activism, parenting support, and more. We depend on one another to see the whole picture.
A few days after the dinner, I attended an interdisciplinary workshop about trauma with philosopher Havi Carel and a range of speakers including philosophers, literary scholars, educators, and a music therapist. Once again, none of us could claim epistemic dominance. Professor Havi Carel is perhaps best known for her work on Epistemic justice in healthcare.
Epistemic injustice in healthcare happens when a professional assumes that because of certain characteristics their patient is an unreliable narrator and interpreter of their own experiences. Consequently they fail to listen to or take seriously what their patient has to say. The only story that counts is the medical history and the only interpretation that matters is the diagnostic formulation. Patients experience not being seen or heard, i.e. invalidation.
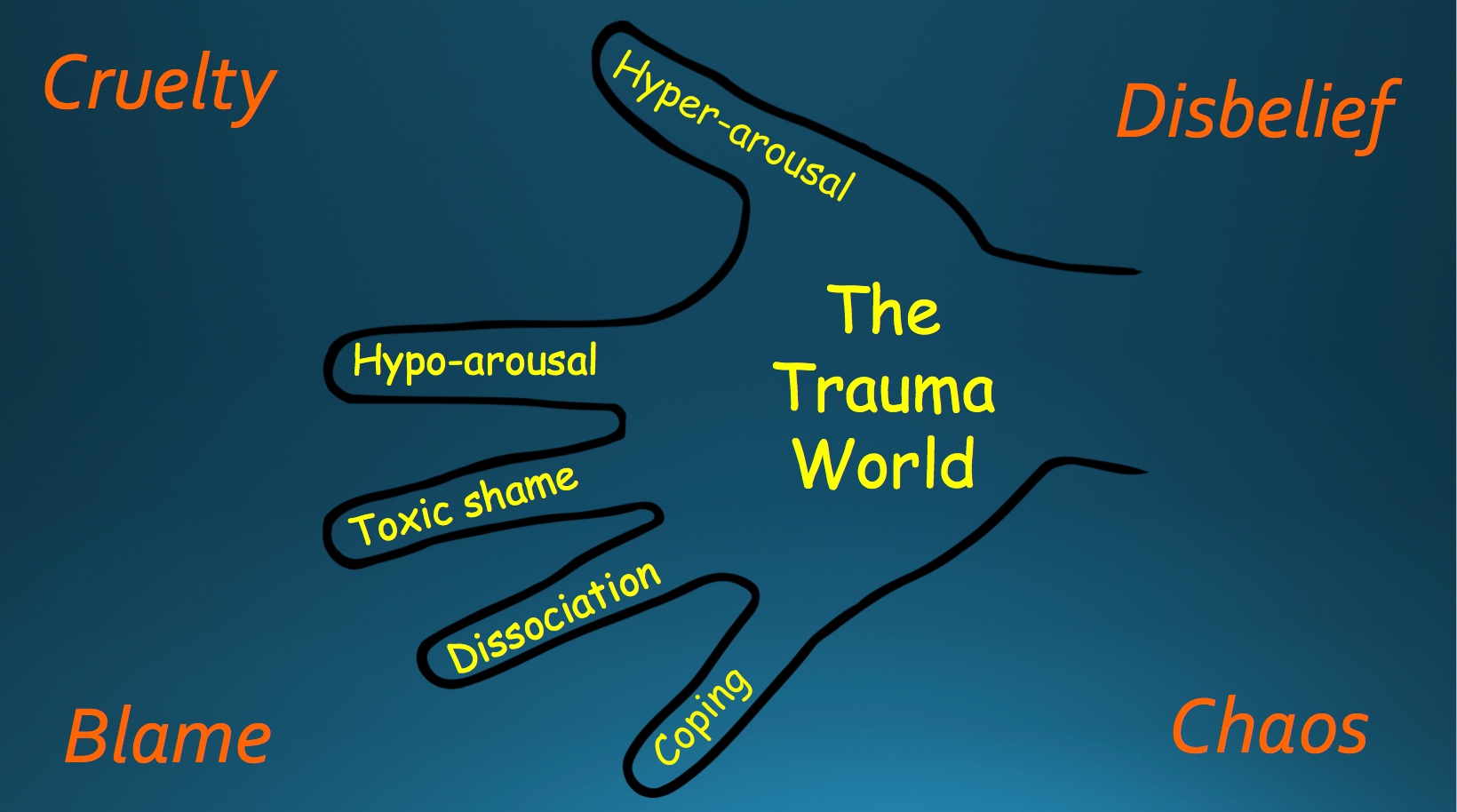
People who are suffering the consequences of trauma, living with what I describe as the trauma world of hypervigilance, shut-down, toxic shame, dissociation and harmful coping strategies, are especially likely to have characteristics that professionals assume render them unreliable witnesses. These include being a child or female or trans, being black or other ethnic minority, being neuro-divergent or having a mental illness, having any kind of physical or mental disability, having an addiction past or present, being homeless, having low levels of literacy or educational attainment and so on. Intersectionality matters, so a Black woman with a mental illness and an addiction is subject to multiple assumptions and is especially vulnerable to Epistemic Injustice.
One of many valid definitions of trauma that I’ve heard from researchers including Bessel van de Kolk and Jacob Ham as well as survivors is,
“Trauma is not being seen or heard.”
Trauma happens under conditions of overwhelming stress where those affected are unable to talk about what’s happening because it is too dangerous or there is nobody who will listen. They learn to bottle it up and in so doing, increase the risk of the kinds of inflammatory and autoimmune disease that are hugely over-represented in people with traumatic life histories. A healthcare professional represents someone with power who may cause the patient to re-experience feelings of powerlessness, but also has the potential to provide a safe environment and attuned presence. If they feel safe enough, patients may want to talk about what has happened to them. If we refuse to listen or don’t listen carefully enough, then they may experience the traumatic invalidation that they have suffered before, and the potential harm is enormous. Patients with trauma are at greater risk of Epistemic Injustice and suffer greater harm from it.
My own Achilles heel as a doctor is explaining too much. I recently discovered a quote from Donald Winnacott, a child psychotherapist and paediatrician who worked near my practice over 50 years ago and it was reassuring to know that we have at least this in common:
“It appals me to think how much deep change I have prevented or delayed in patients in a certain classification category by my personal need to interpret. If only we can wait, the patient arrives at understanding creatively and with immense joy, and now I enjoy this joy more than I used to enjoy the sense of having been clever. I think I interpret mainly to let the patient know the limits of my understanding. The principle is that it is the patient and only the patient who has the answers. We may or may not enable him or her to encompass what is known or become aware of it with acceptance.” From Playing and Reality
In my teaching about trauma, I use a quote from Leslie Jamieson, The Empathy Exams:
“Empathy is asking the questions whose answers need listening to.”
I hope to persuade the doctors and students that I teach, as well as constantly reminding myself that you can demonstrate your expertise by the questions you ask. In so doing we can enable patients to tell their stories and come up with interpretations that help them make sense of their experiences. It’s important to remember that figuring why you are like you are doesn’t necessarily make things better, and may even make things worse, but it is a necessary part of a healing process. Making sense of painful lives through stories is not a radical departure from clinical medicine, but an essential and inseparable part of it. Stories are how medical knowledge is transmitted and ‘how doctors think’ even if we’re unaware of it.
In summary, understanding epistemic (in)justice is essential for trauma-informed care because patients affected by trauma are more likely to not be listened to or taken seriously and are more likely to be harmed by invalidation. Because no specialty within medicine can claim epistemic dominance, they experience what Psychoanalyst Michael Balint described as the ‘collusion of anonymity,’ where “the patient is passed from one specialist to another with nobody taking responsibility for the whole person.”
The answer for me lies in creating a safe environment and continuity of care with well cared-for and respected generalist professionals who can truly listen.
Thanks to Flo, who has been helping me teach this and has inspired me to try to figure this out.
On the psychological level recognition means support. As soon as we are ill we fear that our illness is unique. We argue with ourselves and rationalize, but a ghost of the fear remains. And it remains for a very good reason. The illness, as an undefined force, is a potential threat to our very being and we are bound to be highly conscious of the uniqueness of that being. The illness, in other words, shares in our own uniqueness. By fearing its threat, we embrace it and make it specially our own. That is why patients are inordinately relieved when doctors give their complaint a name. The name may mean very little to them; they may understand nothing of what it signifies; but because it has a name it has an independent existence from them. They can now struggle or complain against it. To have a complaint recognized, that is to say defined, limited and depersonalized is to be made stronger. John Berger
“Illness is what you have when you go to the doctor, disease is what you have when you leave” Iona Heath.
There is an interlocking Venn diagram of illness, disease, and sickness, first proposed by Andrew Twaddle in 1968. Illness is a subjective sense that there is something wrong, you don’t feel well. Disease is the physiological or biological dysfunction. You can have illness without disease – a headache or backache or fatigue for example, or disease without illness – cancer or kidney disease without any symptoms. Sickness is the social identity/ social life of the illness and/or disease. In the case of Diabetes for example, illness may be symptoms of fatigue and thirst, disease includes insulin depletion and insulin resistance, and sickness involves having to take medication, attend GP and hospital appointments, calorie counting and glucose monitoring.
Sociologist of diagnosis Annemarie Jutel describes diagnosis as a medical superpower because of its transformative potential. Citing examples from fiction, like Walter White in Breaking Bad who is transformed from High School chemistry teacher to murdering drug lord by his diagnosis of lung cancer, to a neurosurgeon disarming an assailant by the act of diagnosing him with the same terminal condition that affected his father in Ian McEwan’s book, ‘Saturday’. Because of its transformative power either to change or reveal a true identity underneath, a diagnosis is a common literary device.
Whereas most diagnoses follow illness and offer a medical explanation for symptoms that patients are suffering, there are some diagnoses that are given to people who hadn’t considered themselves to be ill. Danielle Spencer defines a ‘metagnosis’ as a diagnosis of a condition that has always been there, for example when neurodevelopmental conditions like autism or ADHD are diagnosed in adulthood. She describes this transformative power as a ruptured narrative because the story of your life must be rewritten in the light of the explanatory power of the diagnosis.
It is important to note here that illness is seamless, the borders between illness and wellness are fuzzy and indistinct. Diagnoses by contrast are categories with borders guarded by doctors who have the power and authority to give them and on occasion, to take them away. This is one of fundamental problems with the diagnostic project. It began in the 17th century based on natural classifications of animal and plant species, but diagnoses are not natural categories. With the exception of genetic disorders and some other inherited disorders, they are defined by committees of experts, frequently contested, occasionally revised, sometimes redacted, and can only be authorised by medical professionals. They are social categories, not facts of nature.
This is not to say that diagnoses lack any validity or reliability. Validity is the accuracy with which a diagnosis defines and differentiates a diagnosis from other disorders, reliability is the consistency with which a diagnosis is applied between different professionals and over time. A diagnosis needs to be both valid and reliable and professional judgement is relied upon to ensure that diagnoses are not applied arbitrarily so that validity and reliability are assured. Medical professionals are trained diagnosticians.
What are diagnoses for? Competing and conflicting functions.
One way of thinking about this is in terms of micro, meso, and meta functions.
At the micro level, there is the point at which your illness is diagnosed. As in the quote from John Berger at the beginning of this essay, to be diagnosed is to have your suffering validated. And I think it matters a lot that there is an imbalance of power between doctor and patient because validation from a doctor means being seen and heard and believed and taken seriously by someone in a position of authority. It serves as an explanation and serves a moral function – “It’s not me, it’s the illness”. To be told that your results have all come back normal and your symptoms do not amount to a diagnosis may not result in relief, but may be perceived as disbelief, and experienced as invalidation. In these cases patients who feel ill and are suffering but not diagnosed say that they feel ‘fobbed off’. Disbelief and invalidation from a powerful figure may trigger memories of other times in a patient’s life when someone in power or authority over them didn’t take their concerns seriously. In some cases this transference can put the doctor in the symbolic role of an abusive partner or neglectful parent.
At a meso level diagnosis serves as a way of professional communication, shorthand to accurately describe a condition, ensuring that the right treatment is used, safely and appropriately for the condition that it was tested on before it was licensed and approved to be prescribed. Researchers need to know that when they are testing a treatment for migraine in one study, they are treating the same condition that was being treated in other migraine studies. Clear, valid and reliable diagnostic categories enable epidemiological studies to track the numbers of people with different conditions and their rise and fall and response to social, environmental and other factors. A diagnosis can make the invisible visible, for example in my practice we have tried to identify and code everybody with chronic pain, so that we know what proportion of our patients have chronic pain and can be sure they are receiving appropriate treatment. If every practice did this we could lobby for more training more resources and more support for people with chronic pain and those who look after them. For research and epidemiological studies, tightly defined diagnostic categories are especially useful here, at the meso level, whereas at a micro level they are more loosely applied.
At a macro-level diagnosis serves social and administrative purposes. So instead of trying to describe symptoms you can simply say, “I’m having a migraine” or “it’s the menopause” or, “I’ve been diagnosed with lung cancer” and people will give you peace and quiet, empathy or sympathy accordingly. A diagnosis enables access to benefits, adjustments at school, in exams and at work, and sick leave. It allocates and rations treatment, so that services can focus on the people who really need their help and are likely to benefit from it. Treating people who are depressed but do not have a major depressive illness with psychotropic drugs is likely to do more harm than good. Treating people with all degrees of ADHD with the same medications and adjustments at work and college disadvantages those at the more severe end of the spectrum as well as those with similar difficulties who have not been diagnosed.
Self-diagnosis.
Self-diagnosis has become vastly more popular since I qualified as a doctor in 1996 for a number of reasons including, but probably not limited to, the internet, social media, politics and individualism, scientism, direct to consumer advertising, and the loss of belief in expertise. The internet enables everyone to look up their symptoms online and AI will even do that for you. Social media enables ‘influencers’ and advocacy groups to coalesce around shared identities to much greater extents than in the off-line world of shared interests, geographies, purposes or projects. Political neoliberalism over the course of my personal and professional lifetime has moved away from issues of class and justice towards individualism, identity and rights. Scientism which is the dogma that purports that science (and especially medical science) is the truest way of explaining the world, has meant that people increasingly describe social problems in medical / psychological language, so that social challenges get described in terms of individual anxiety, depression or complex trauma. Direct to consumer advertising of drugs and diseases creates demands for medication or diagnoses that confer a right to treatment (in many cases drugs). There are many ‘advocacy groups’ for diseases funded by drug companies for example. And the loss of belief in expertise, or perhaps the loss of epistemic authority has empowered patients to be their own diagnosticians.
Self-diagnosis is concerned with the micro and macro level uses of diagnosis, but not so much with the meso level, where strictly controlled boundaries are more rigorously applied. As a GP I too have little to do with the meso level, but I am concerned to preserve the validity and reliability of diagnoses and ensure that my patients get the appropriate treatment and aren’t harmed by an inappropriate diagnosis or none where one is appropriate.
Like many doctors, I am confronted by increasing numbers of patients looking for me to confirm the diagnosis they have already diagnosed themselves, from parasitic infestations, to chronic Lyme disease, ADHD and autism, the andropause and more. There are apparently ‘affirmative diagnostic services’ operating privately, although it’s long been known that you can get almost any diagnosis if you pay the right doctor. The risk here is of a heuristic known as a ‘confirmation bias’, whereby alternative explanations are overlooked. One patient came in wanting a diagnosis of ADHD for no reason they could identify other than, “I want to know why I am like I am”. I thought that they should see a therapist, or travel or read (or take hallucinogenic drugs or whatever), but it wasn’t existential soul-searching they were looking for, it was a diagnosis. For some people a diagnosis gives them access to a group with the affiliation and validation that goes with membership. Loss of that group identity can be distressing. I have one patient whose psychiatrist revised her long-standing Bipolar diagnosis which meant that she could no longer go to her Bipolar support group that she had been going to for years and it was far more upsetting than liberating. I know a once prominent Chronic Pain patient advocate/campaigner who recovered and was ostracised from her group, and treated as a pariah. A diagnosis can be sticky especially when it’s taken on as an identity. The son of a friend who has moderately severe autism insists that he doesn’t want it to define him while there are others whose autism would be impossible to spot we’re it not for their out and proud self identification.
As an NHS GP, patients do not pay me for a diagnosis. I have to preserve my clinical integrity and protect my patients. I’m their doctor always and their ally when I need to be.
Psychiatrist philosopher Chloe Saunders gives 3 reasons for being concerned about self-diagnosis
Epistemic authority of clinician necessary for meaningful diagnosis
Diagnosis has many competing functions.
Potential harms: “I have/ am X, therefore Y
If patients were able to diagnose themselves, they wouldn’t be upset so often as they are when a doctor doesn’t agree with them. There are quite frequent disagreements over psychiatric diagnoses like bipolar and ADHD, but also relating to male menopause and symptoms of chronic pain or fatigue which patients prefer to attribute to a diagnosis. Not infrequently, because I work in a deprived area where a lot of my patients depend on benefits, the social, bureaucratic function of diagnoses means that whether or not my patients’ symptoms can be described in terms of a diagnosis means the difference between getting enough benefits to be able to afford to eat or not. The pragmatic GP finds a way to label symptoms in a way that stops their patients from starving. This is the state of deprivation in England today.
A diagnosis can serve as bureaucratic shorthand, but it’s also shorthand for patients too. It can explain their difficulties more succinctly and with less self-examination than psychodynamic therapy. This is not to say that a diagnosis necessarily serves to close off other ways of thinking, but it’s certainly a risk, and ‘diagnostic overshadowing’ is something patients as well as clinicians are concerned about. A misdiagnosis, for example, if a patient diagnosed with ADHD instead of bipolar disorder might result in a manic psychosis being triggered by stimulant medication.
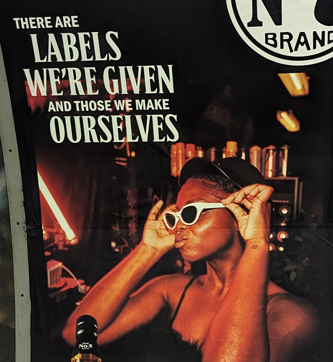
The competing functions of diagnosis I’ve outlined above. There are overlaps between diagnosis and identity and when patients strongly identify with their diagnosis it shape who they are and who they become and serve to explain aspects of their personality and behaviour that may not be helpful. The mantras, “I am not my trauma” and “history is not destiny” are important ones in the area of Complex PTSD and developmental trauma, but can be applied in all aspects of mental health where nihilism can trap people inside the identity of their diagnosis. The mantras exist, because there is the tension between illness and identity is very hard to resolve. In his essays on the diagnostic classifications for the London Review of Books, Ian Hacking described ‘Looping Effects’ and ‘Making People Up’. The act of creating classifications of certain kinds of people changes these people and this is the ‘Looping effect’ “Sometimes our sciences create kinds of people that in a certain sense did not exist before. I call this ‘making up people’”.
He proposes two sentences, (I paraphrase slightly)
There were no people with this disorder before it was defined and given a diagnosis.
Before the diagnosis of this disorder, people did not experience themselves this way. It was not a way to interact with their friends, family, employers, but after the disorder was defined and given a diagnosis it was a way to be a person, to experience oneself, to live in society.
His argument is that disagreements over 1 don’t get us very far. Whether or not you think that ADHD exists or is a specious diagnosis, will likely never be resolved. What we can (hopefully) agree on is that it is now a way of existing in the world in ways it wasn’t before as a result of the creation of the diagnostic category. 2 is true.
The tension between illness and identity is very well described in this personal account of depression, Am I Blue? There is a tautological trap, or Mobius strip of circularity when she asks herself “why am I depressed?” and the answer circles around various possible causes before coming back to, “because you have depression”. Is depressed something you are or depression something you have? Is a question that’s very difficult to answer, because mental illness transforms identity.
Philosopher Havi Carel talks about existential and epistemic transformation of illness. Take Mary and Martha, women in their 60s who had heart attacks at the same time. Both were patients of mine and had lived pretty rough Hoxton lives which featured a lot of cigarettes, alcohol and violence. I visited both of them shortly after discharge from hospital. Mary told me that she had been meaning to sort her life out for some time, and surviving this heart attack convinced her that if she didn’t do it now, she would likely die. She left her husband, gave up alcohol and cigarettes, changed her diet and spent her days volunteering at her church. Martha said that she wasn’t going to let a heart attack change a thing and carried on with the same lifestyle as before. Both Mary and Martha were epistemically transformed because they had first person knowledge of a heart attack and heart disease that you cannot get without suffering it yourself. Perhaps only Mary was existentially transformed, however Martha, for all her insistence that a heart attack wouldn’t change her, experienced the world differently after her heart attack. She continued to get angina and this exacerbated her anxiety, she got breathless and these both restricted her physical activity and constrained her social life. She became increasingly withdrawn and died a couple of years later from another heart attack. Mary still comes to see me and reminds me of how much her life has changed.
Diagnoses and Identities are evolving all the time.
I think that many of the problems described above are because identities aren’t fixed, and as writer Rebecca Solnit says, “all categories are leaky and provisional”. I think the same about identities. I’m 52 and pretty comfortable these days accepting the ways that my injuries have shaped my body, my children have transformed me in ways I can’t begin to describe, work affects my mental health and self-esteem, my familial genes, traits and experiences continue to affect me, as much as ever, and the illnesses and life stories I’m exposed to infect me and affect me. The search for an authentic identity underneath it all is like peeling an onion, there are layers and layers and then nothing.
As a pragmatic GP hanging on to clinical integrity in the later years of my career, it’s still part of my job to help patients make sense of their experiences in the light of all the available evidence and to offer my clinical judgement rather than acquiesce to diagnostic affirmation. After all, diagnosis is a medical superpower, and as Spiderman’s uncle Ben says, “With great power, comes great responsibility”
When I get sick, I want to be looked after by someone who enjoys their work, is motivated, up to date, and well supported. Someone whose work gives meaning and purpose to their life. I want someone who is driven by desire to look after me and make me better, who enjoys figuring out diagnostic dilemmas and sharing treatment options. I want someone who is interested in my illness and cares about me because healthcare is about people caring for people.
The biggest barrier to this kind of care, is demoralised, alienated healthcare staff.
The latest GMC (General Medical Council) State of Medical Education and Practice report published in June 2023 concluded that more doctors than ever are at risk of burnout, are considering leaving the profession, and have experienced compromised patient safety or care. I’m afraid that if I do get sick, I’ll be looked after by someone like this.
While it’s tempting to believe that there was a ‘golden era’ where NHS staff were overwhelmingly enthusiastic and caring, the reality is that healthcare professionals have rarely, if ever been treated in ways that fully enable them to give the best possible care to their patients.
Long before the NHS began Karl Marx described four aspects of alienation that affected workers under industrial means of production: alienation from the process of labour; alienation from the products of labour; alienation from themselves and alienation from others. And in 1959 Isabel Menzies Lyth described attempts by managers and senior nurses to deal with burnout in nursing students that made the problems worse by further alienating the students in the ways that Marx described. In 2023 it seems clear to me that alienation is the problem affecting healthcare professionals in the NHS today, and attempts to deal with burnout and stress are making things worse in the same ways that Menzies Lyth observed over 60 years ago. I’ll focus on GPs for the reason that I’ve been a GP for over 20 years, but I think the problems apply to all doctors and many other healthcare professionals.
Alienation from the process of labour
The basic process of labour for a GP is a clinical consultation where I want to offer my full attention and presence to someone who may be overwhelmed by illness and stress. I want the organisation and IT to support this, so that I have enough time and we are uninterrupted, I have all the information I need and the tools of production – equipment, as well as access to investigations and clinical colleagues are all available, and the IT works perfectly, or at least adequately.
For Marx, alienation from the process of production meant that workers feel they lack control over the conditions of their work, and they are pressured to prove that they are being productive, with rewards for success or punishment for failure despite them having little or no autonomy. The reality for most GPs is that very frequently lack the time they need with patients, are frequently interrupted, and lack access to the tools they need (especially support). Instead of supporting them to do their work, the IT demands data entry above all else and seizes up or slows down all the time. We are judged and therefore paid, above all else according to efficient data entry.
According to Marx,
“The worker “[d]oes not feel content but unhappy, does not develop freely his physical and mental energy but mortifies his body and ruins his mind. The worker therefore only feels himself outside his work, and in his work feels outside himself;” The production content, direction and form are imposed by the capitalist. The worker is being controlled and told what to do since they do not own the means of production, they have no say in production, “labour is external to the worker, i.e. it does not belong to his essential being.”
The recent Commonwealth Fund report into General Practice showed that job satisfaction was lowest in the UK of all countries surveyed, especially with regards to workload, administrative burdens and time available to spend with patients.
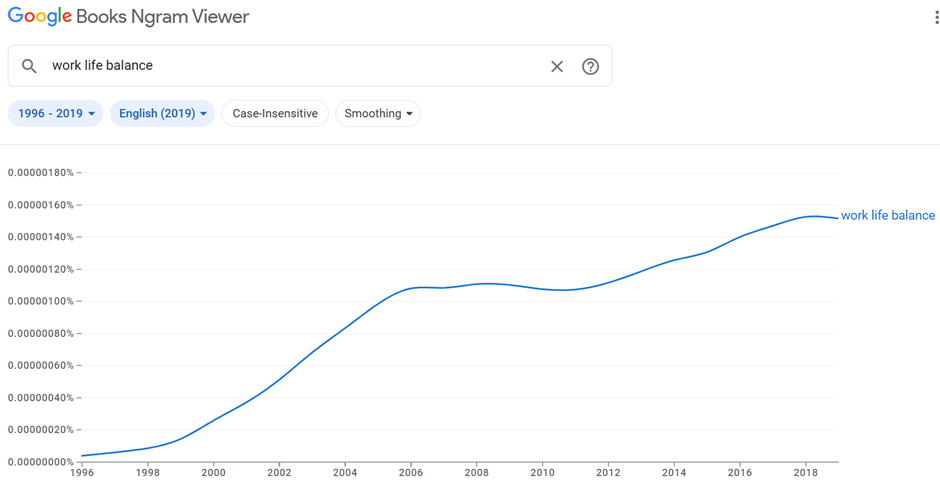
Lacking meaning, purpose and satisfaction in work, workers seek these things elsewhere. Many doctors are choosing ‘portfolio careers’ with only one role in the NHS and others in private medicine or other careers entirely. Doctors these days are told to consider their work-life balance as if work is not part of life, but something they are obliged to do in order to earn enough money to have a life elsewhere. I qualified as a doctor in 1996 and this is the rise in use of the term ‘work life balance’ according to Google.
When work has meaning and purpose and when workers have adequate degrees of autonomy, control and responsibility over their working conditions, then the issue of ‘work-life’ balance becomes less of an issue, because work is part of life.
Breaking down something complex and relational like a consultation into an opportunity for data entry is a form of ‘taskification’ described by Professor Alison Leary, in her excellent presentation for the Nuffield Trust (19.02). ‘Taskification’ is an aspect of industrialisation described by Taylor (1882-1911) Taylorism was a method for increasing the productivity of industrial work. Also known as scientific management Taylor broke work down into standardised tasks, with workers paid according to complexity, working at the top of their grade/ limit of their skills, with rewards for success and loss or punishment for failure. In healthcare jobs have been broken down into tasks which must be meticulously and repetitively documented. Tasks that are considered more straightforward are given to qualified, less well-paid people. There are now over 7000 different roles in the NHS forcing staff to spend more time working at the top of their grade while new roles take on work they used to do. When I started working as a GP, a ’pill check’ was a consultation where you met a woman to check her blood pressure and discuss how she was getting on with her contraceptive pill. ‘Pill check’ was shorthand for catching up in a clinic that was running late, recovering a little between consultations that were emotionally draining or clinically complex. Almost every consultation resembling a ‘pill check’ is now done by someone else, so we find ourselves doing more demanding work without respite.
Alongside our clinics full of complex patients GPs are responsible for everyone else that is seeing the patients that we used to see, like sick children. This is relatively simple in terms of clinical decision-making, but valuable and enjoyable work and gives GPs an opportunity to build relationships with young families. Often the supervision takes more time than it used to take when the GP saw the patient. As Spike Milligan joked in the 1990’s, “I’ve invented a machine that does the work of two men, but it takes three men to operate it!”
Taskification also describes the demands that the electronic medical record (EMR) places on clinical encounters. At one time a useful place to document my thoughts, the EMR has become a behemoth of dashboards and I have become a data-entry slave while my patients and colleagues are starved of my attention. Trying to find details about a patient’s life circumstances which are essential to make sense of symptoms and suffering is almost impossible among the pages of templates in which tasks are documented. Patients meet anonymous professionals who fill in checklists instead of caring professionals who can give their full attention.
In 1959, Isabel Menzies Lyth was asked to investigate a London teaching hospital where nearly 40% of student nurses were quitting before completing their training, a proportion not seen since, until very recently. She was writing at a time when professional knowledge was shrouded in secrecy, paternalism was unquestioned and external scrutiny was frowned upon. Sixty years later, Don Berwick, head of the Institute for Health Improvement, described this as Era1 for medicine. According to Berwick we have responded to this with Era 2- “A massive ravenous investment in tools of scrutiny and inspection and control, massive investment in contingency and massive under-investment in change and learning and innovation”
The collision of norms from these 2 eras—between the romance of professional autonomy on the one hand, and the various tools of external accountability on the other—leads to discomfort and self-protective reactions. Physicians, other clinicians, and many health care managers feel angry, misunderstood, and overcontrolled. Payers, governments, and consumer groups feel suspicious, resisted, and often helpless. Champions of era 1 circle the wagons to defend professional prerogatives. Champions of era 2 invest in more and more ravenous inspection and control.
There is little point telling health professionals, who are committed and conscientious, that they have nothing to fear from inspections. My own consulting room breaks all kinds of rules for having a hand-woven rug on the floor, plants on the shelves and edible products in the drawers. Nobody from CQC has ever inspected my patient interactions, my clinical supervision, or my open-door policy for students, trainees and colleagues.
Alienation from the products of labour
Alienation from the products of labour occurs when clinical staff are unable to relate to the results of their interventions on individual patients because their involvement is so brief, so partial, and they aren’t involved in follow up. For Marx, the worker should be able to see something of himself in the final product. An example of delayed gratification in this respect is a story told by a doctor in an episode of The Nocturnists podcast where Emergency Physician Mike Abernethy described the impact of meeting a patient whose life he saved thirty years before, while shopping in Walmart. Listening to it I sensed the alienation he felt from not knowing at the time of his involvement whether the child he had operated on had survived. Discovering that he had grown to be a healthy adult 30 years later, the emotional impact of feeling a sense of connection with the product of his labour is immense.
Having a relationship with the products of your labour – a patient who recovers or one who does less well is essential for learning as well as finding meaning and purpose in work. Being reduced to a cog in a machine is demoralising. GPs are paid for the quality and quantity of their data collection because this is easier to measure than the products of their labour – patients with healthier lives. Even surgeons whose relationship with the products of their labour is more straightforward are contractually sometimes unable to follow up their patients for long enough to know much if anything about the long-term impact of their work.
Alienation from ourselves
We are alienated from ourselves because the values that bought us into clinical practice and are part of our professional, caring identity are crushed or compromised by our experiences. Professor Jill Maben described the erosion of idealism among nursing students in 2007. Lacking the time or resources to make a difference or provide the care that we know their patients need, we suffer moral injury.
In 1959, Isabel Menzies Lyth described institutional ‘defences against anxiety’ which demoralised nurses in a London teaching hospital. They were given very little autonomy and not allowed to take responsibility even when they were capable. A risk averse culture meant that even trivial decisions had to be passed up to senior staff and everything had to be documented, often multiple times. The nurses came into their profession with ideals of caring and being cared for in a caring culture and discovered that this was almost impossible, and consequently they were overwhelmed and anxious. Management believed that their anxiety stemmed from having to deal with patients with serious illness who were sometimes dying and often in abject states – having to deal with the visceral reality of bodily fluids and infection and incurable disease. To ‘protect’ nurses from the emotional labour of their work, management and senior nurses broke up the relationships that developed from individual patient care so that nurses instead were responsible for tasks such as patient observations, medication rounds, admissions, discharges and so on. These decisions were misguided because emotionally demanding though the work was, it was what the student nurses had chosen to do. Rather than help them cope better with it by providing support, policies separated them from the meaningful aspects of their work. As a GP with interests in complex trauma and chronic pain, I know that, as Anatole Broyard wrote,
“Physicians have been taught in medical school that they must keep the patient at a distance because there isn’t time to accommodate his personality, or because if the doctor becomes involved in the patient’s predicament, the emotional burden will be too great. As I’ve suggested, it doesn’t take much time to make good contact, but beyond that the emotional burden of avoiding the patient may be much harder on the doctor than he imagines. It may be that this sometimes makes him complain of feeling harassed. A doctor’s job would be so much more interesting and satisfying if he simply let himself plunge into the patient, if he could lose his own fear of falling.”
One principle when helping patients cope with the aftermath of trauma is that attempts to escape the resulting hypervigilance, numbness and pain, shame and guilt, often through the use of alcohol or drugs, binge-eating or other addictive behaviour – does more harm than actually working with trauma’s physical and psychic wounds. Doctors who find themselves feeling overwhelmed by the impact of patient suffering need to be supported to lean in and have more effective therapeutic relationships rather than keeping their patients at arm’s length.
Alienation from others
In his latest book, The Distance Between Us, Darren McGarvey proposes that the major problem in Britain today is that the ruling class and the working classes are so alienated from one-another that they cannot possibly understand each other’s experiences, values, needs or motivations. Alienation from colleagues in healthcare also results from intensely busy shift work culture that makes it very difficult for colleagues to meet with each other to discuss their work or even get together and go out and relax after work. Shifts for junior doctors and GPs may be shorter than they used to be, but they are so pressured that there are very few opportunities to know what others are dealing with. We’re glued to our computers. Supervision becomes perfunctory and education becomes didact, “do this, don’t do that” rather than a thoughtful discussion. There’s no time for small talk, no checking in to see if colleagues are coping and few people have any capacity to lend a hand. People, specialties, departments and organisations defend their boundaries fiercely with referral protocols. Only half-jokingly do we say our patients are either too mad, not mad enough or the wrong kind of mad for any of the available mental health services. Online meetings have obliterated time spent travelling and eating together or sharing a coffee and catching up. Small talk, which has always been an invaluable way to share knowledge and support one’s colleagues is severely endangered.
Alienation is as much an issue today as it was when Marx described it in 1844 and when Menzies Lyth wrote about it in 1959.
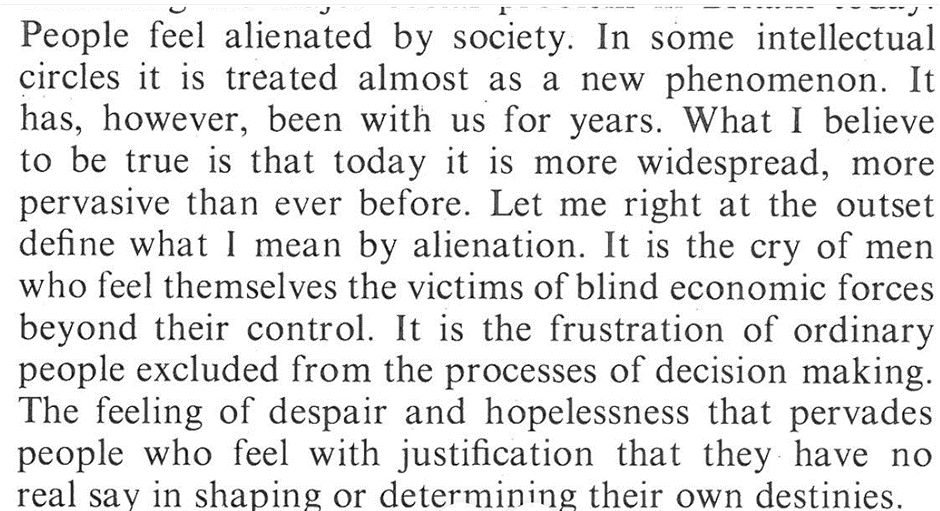
In 1972, James Reid, rector of Glasgow university gave his inaugural address,
From alienation to connection.
The cure for alienation is connection, connection with the processes and outcomes of our work and connection with our colleagues and ourselves. We need the time, support and resources to do our work to the best of our ability, so we need to invest in more and better administrative support and IT that actually supports effective consultations. In Era 3 for medicine, Don Berwick calls for a 70% reduction in clinical admin over 5 years. This alone would improve retention of GPs above anything else. Connection with the outcomes of our labour requires organisations to focus on relational continuity and whole-person care so that GPs can learn alongside their patients about how illness interventions impact them over time. Connection with our colleagues needs to be valued and time for informal support as well as formal opportunities for supervision and education needs to be paid at the same rate as clinical duties. Connection with our ideals needs organisations and policy makers to understand what gives GPs meaning and purpose in their work and support this in every possible way or they will leave to work elsewhere or change career. In the immediate term, the biggest risk is that doctors will leave the most stressful work, which is, and has always been among patients experiencing the highest levels of deprivation. They will reduce their hours, or leave to work in less deprived areas, or overseas or to do private work. The Inverse Care Law states that the supply of healthcare is always inversely proportionate to the need for care, and more so wherever market forces influence the supply. As philosopher Michael Sandel warned, we have moved from a situation where market forces aren’t just used to shape the economy, but are used to influence everything in society, including healthcare.
Attention to alienation and connection could be the cure that the NHS needs.
In 1996 I was newly qualified. I had completed my training as a doctor without being taught anything about chronic pain. As a junior doctor, how to do medicine was my overwhelming concern and this mostly meant knowing the rules and the protocols and sticking to them. Samuel Shem’s book the House of God was our guide to when and how to break rules to protect ourselves from the toxic culture, our seniors and the patients. The House of God’s Golden Rule was ‘do as much nothing as possible’ which was an explicit acknowledgement that hospitals are dangerous places where all interventions are risky, but almost any intervention can be justified, meaning many patients would be better off if they were sent home, perhaps with some extra social care rather than risk medical interference. Patients were referred to as GOMERS which stands for Get out of my emergency room. Patients with chronic pain encountered in Emergency rooms or A&E departments were GOMERS and we did what we could to turf them. Turfing means sending them home or referring them to another specialty. This being the mid 90’s the department had a cupboard full of little boxes of Tramadol kindly provided by a pharma rep. and it was a quick and easy way to send someone home, with a new potent painkilling drug that we had been assured was more effective, safer and less addictive than pretty much anything else at that time. It made our lives easier and so we didn’t question it. Our involvement with patients with chronic pain was so transient that we had little sense of the chronicity of their pain and even less of their lives.
As I rotated through different hospital specialties there were a few occasions where I encountered patients with chronic pain. I remember a woman whose stomach was criss-crossed with surgical scars where surgeons had repeatedly explored her abdomen and pelvis looking for the cause of her pain, until eventually the internal scarring became a cause of pain in and of itself and they stopped looking.
Patients like this were frustrating to their surgeons, to put it mildly, but more bewildering than frustrating to me because I felt less responsibility for their recovery. I think that this is one reason why patients with chronic pain sometimes experience more empathy and sympathy from medical students and junior doctors than experienced clinicians. Once we start to feel more responsible for our patients’ recovery things get more complicated. People become doctors because they want to make a difference by relieving suffering. Writing in 1959 about doctor-patient and nurse-patient relationships, the psychoanalyst Thomas Main, noted that if this desire to relieve suffering is not satisfied, “they tend to become more passionate, to be reinforced with aggression and then to deteriorate in maturity, with sadism invading the situation.” I knew a gynaecologist whose attitude towards her outpatients – about 50% of whom have unexplained pelvic pain, verged on the vengeful. Writing about nurses caring for patients in pain Main noted that “[she] would only give a sedation at the moment when she had reached the limit of her human resources and was no longer able to stand the patients problems without impatience, anxiety, guilt, anger, or despair”. The use of sedatives went up, the more understaffed and stressed the nurses were. These days we know that GPs prescribe more opiates where there are fewer GPs, less continuity, and shorter appointments. In these situations, medications are more available and dependable than doctors.
For many doctors, especially those working in hospitals, or those in general practice without the long-view, favourite patients are often those who massage their ego, whose diagnosis or treatment is a bit of a challenge, who recover from serious illness, ideally after a bit of a battle, and are grateful for it. Patients with chronic pain are rarely like this because recovery is not in their repertoire and they are usually as frustrated by their lack of progress as their doctors. On those rare occasions when they do recover, they are among doctors’ most favourite of all because the battle has been so long and hard-fought and also involves an interesting quest or journey.
Medical sociologist Arthur Frank described three kinds of illness narratives. The classic restitution narrative follows a satisfying illness-diagnosis-treatment-recovery trajectory. A quest narrative involves a coming-to-terms with a long-term condition and a journey of acceptance; “Quest stories carry the unavoidable message the restitution narrative will, one day, prove inadequate”. A doctor likes a patient on a quest because they’re no longer pestering them for a cure but sharing updates from their travels. The third kind of narrative, and the one that typifies chronic pain, is chaos. People live in chaos, but, says Frank, “chaos in its purest form cannot be told” Chaos tears up narrative. Listening to patients in chaos is hard to follow, there’s a very real sense of going nowhere. Philosopher John Berger wrote that patients who suffered without a diagnosis couldn’t separate their illness from themselves, but a diagnosis gave their illness an independent existence so that doctor and patient could struggle together against it. Chronic pain is a kind of diagnosis without diagnosis, there’s nothing to show on the scans or blood tests. In chaos, there is no thing to be treated, or cut away, there’s nothing like cancer to provide an explanation, attract sympathy or entitle benefits. Patients in chaos can be deeply frustrating for doctors because they’re repeatedly confronted by suffering and reminded of their failure to make a difference. Writer Hilary Mantel, who suffered with chronic pain wrote of her,
“concern with the doctors and nurses who have to deal with patients who are in pain, I think it must be a depressing and unsettling business unless you are well-trained and supported.”
And of course we are not well trained in chronic pain and we’re even less well supported. Like Thomas Main 50 years before, she experienced that frustrated medics can be callous.
A lot is made of studies that show that medical students lose their empathy as they go through medical education. This is because they learn to listen before they learn to diagnose and they learn to diagnose before they learn to treat. By the end of their training they listen selectively, if at all, mostly to make a diagnosis and set up the treatment protocol as quickly as possible. But as students, to begin with at least, they listen without judgement, without steering the conversation towards a diagnostic end point. Being under no pressure to make a diagnosis or relieve their patients’ symptoms, and given much more time than doctors, patients are often more at ease with students and in my experience, rate them highly for listening. The experience of being seen and heard is validation – and the importance of validation is the most consistent finding of all the studies looking at the experiences of patients with chronic pain in their interactions with medical professionals.
In the documentary, Cracked Up, Actor and comedian Darrell Hammond described trauma as ‘not being seen or heard’. Invalidation from healthcare professionals is traumatic, worsening the isolation, shame and self-doubt that so often accompany chronic pain. One question doctor and patient may have, but rarely admit is, ‘what role is trauma playing here?’ It’s not a question of root causes, but if I can stick to the analogy of actors depicting chronic pain, there will be many, and trauma will play their role, alongside a cast of others including the careless driver, the anxious mother, and the incident with the stepladder on the ice. Potent as a medical student’s validation may be, validation that comes from someone more powerful than the patient has an added potency, and where there has been childhood trauma the impact of validation from a powerful adult can be revolutionary. Clinical judgements are inescapably moral because some patients are found more worthy of medical care and concern than others. The fear of being labelled or treated as a fraudster or malingerer is ever present. Medical sociologist Daniel Goldberg found that chronic pain sufferers rate the alienation they experience from their physicians as qualitatively worse than alienation from loved ones.
If not being believed is one concern that patients have, another is that of being of little interest to their doctors. Anatole Broyard wrote of his duty to be an interesting patient,
“I would also like a doctor who enjoyed me. I want to be a good story for him, to give him some of my art in exchange for his. If a patient expects a doctor to be interested in him, he ought to try to be interesting. When he shows nothing but the coarser forms of anxiety, it’s only natural for the doctor to feel an aversion. There is an etiquette to being sick. I never act sick with my doctor.”
Broyard was a writer, a critic, an American who had enjoyed robust health until he got prostate cancer. He was an interesting guy, who played with language for a living. Imagine if you’re uneducated, female, dependent on others to interpret for you, and suffering from an illness that’s hard to describe, hard to diagnose and unsatisfactory to treat. Most of my white, English-speaking patients know of the importance of giving a little to their doctor to sustain my interest, and make me feel as if I’m making a difference. They give a little, but also remind me that they don’t dare tell me how bad it really is, they don’t like to disappoint me … too much. It’s not unusual for them to admit that they’ve been afraid to tell me just how awful it has been, what terrible things they’ve sunk to in order to cope, how acutely suicidal they’ve been. But my Turkish and Bengali patients appear to believe that the best way to keep me engaged is to insist, every time they see me, that everything hurts more and nothing works, apparently unaware of Thomas Main’s warning that a despondent, frustrated doctor will at best lose interest and at worst become mean and sadistic. A doctor wants at least a little bit of a quest in their patient’s chronic pain narrative to sustain their interest. Frank understood the challenge for doctors was how to honour the telling of chaos while leaving open a possibility of change; to accept the reality of what is told without accepting its fatalism”.
How I respond to patients with chronic pain has changed over the years. John Berger wrote about Doctor Sassall in his book, A Fortunate Man; “Thriving on medical emergencies, impatient with non-specific symptoms and the absence of clear-cut physical diagnoses and underlying pathology, he moves gradually towards and empathic listening and companionship with his patients and their families, striving to recognise who they are and the meaning of their illness to them. Physical and psychological intimacy is central to his relationship to his patients”.
These days I have consultations where patients come in with chronic pain and leave, after a time, with less pain that is a little easier to bear. This depends on my availability, or presence, which I would like to conclude this essay exploring.
Anatole Broyard wrote,
“I see no reason or need for my doctor to love me – nor would I expect him to suffer with me. I wouldn’t demand a lot of my doctor’s time; I just wish he would brood on my situation for perhaps five minutes, that he would give me his whole mind just once, be bonded with me for a brief space, survey my soul as well as my flesh, to get at my illness for each man is ill in his own way”
“The barriers to ‘being there’ for our patients are not bound up in red tape … they lie in our presence of mind, our inclination to linger and listen, our rigour to pursue some grasp of the patient’s narrative and thereby catch a subtle signal for help”
There are subconscious barriers to presence. At a physiological level, openness in the presence of another involves neuroception – a neurological mirroring with hypervigilance, tingling, and hypersensitivity, raised blood pressure and heart rate, shallower breathing, tightening of skeletal muscle and slowing of digestion; all subtle changes, but enough in total to create an unease and a desire to bring the consultation to an end, perhaps with another referral, prescription or investigation, anything to buy some time before the patient can come back. Other strategies are for the doctor to stop listening and start pain-splaining, or offering advice. At a psychological level the doctor lacks confidence in his ability to negotiate the electrically charged boundaries around empathy; poised between gift and invasion – between seeing someone as they are and between cracking them open. Chronic pain is like a wound. You can’t change whatever it was that caused the wound, but to help it heal, you may need to cut away the scar tissue so that it heals from the bottom up. Historian of pain, Joanna Bourke, reflecting on her own painful experiences with doctors, observed that it wasn’t that pain was hard to talk about, so much as it pains others to listen to people talk about pain. Doctors have a tendency to dissociate when patients talk about pain, and Broyard feared that his doctor would lose interest and wrote of his need to be an interesting patient and not to act sick. But there is, at the same time, an unspoken need to be seen, beneath the demands for pain relief or another MRI scan there is panic and aloneness. I have on the wall of my consulting room a picture of ‘A woman with attitude’ – a reference to all the women I see who remind me of this whenever they come in. Empathy is an art where the doctor can acknowledge their patients’ capability, vulnerability, courage and terror at the same time as they appreciate the humour that so often accompanies serious illness.
In concluding, doctors are poorly prepared to take care of patients with chronic pain, education is improving, but they are under-supported and there are few organisational or financial incentives for the long-term work care that patients with chronic pain need. If you find a good one, then commit to continuity and nurture the relationship. Find one that believes you but will challenge your shame and self-blame, and be interested enough to explore your stories with you rather than accept them at face value. You will want one who can appreciate the dark and the light side of suffering. Your doctor needs to be accessible and boundaried – better five minutes of whole-hearted presence than a half-hearted half-hour. Above all find one that believes that things can get better, not with false hope or through futile interventions, but by perseverance and imagination.
What can be done right now to save NHS General Practice, in a form that is works for patients, practice staff and taxpayers? What should the new Health Secretary Therese Coffey do about GP access?
First of all she needs to understand what GPs do.
The motto of the Royal College of General Practitioners is Caritas cum Scientia
Professor Keiran Sweeny was a GP who wrote about his experiences of being a patient with cancer and said, Medicine is not solely a technical activity and pursuit, medicine is about understanding and being with people at the edge of the human predicament.
When politicians and journalists talk about general practice they give the impression that they think GPs see two kinds of patients; those with simple problems that they can fix and those with more complicated problems that need to see a specialist. They seem to think that someone else should be able to sort out the simple problems and perhaps patients should be able to go straight to a specialist. Sometimes I think they cannot quite see the point of GPs. The reality is that on average about 1 in 10 patients are referred, about 2 in 10 are straightforward and the rest are suffering with long-term, intractable problems like chronic pain and chronic anxiety and depression compounded by a range of complex social circumstances and physical illnesses.
More often than not GPs provide holding work, care and presence in the face of enduring, intolerable suffering. The relationships are where the medicine happens, the GPs are the theraputic agents
So what needs to happen to save NHS General Practice? What should the new Secretary for Health, Thérèse Coffey do now?
1.Access to GPs is best when the right person helps patients at the right time. This depends on excellent clinical and administrative triage from people who know the patients, the practice and the community. Since introducing this at my practice, we have continued to ensure continuity of care at the same time as enabling every patient who contacts the practice an appointment within 2-3 days.
2. Access to GPs is best where health needs are least because the wealthiest areas tend to have the healthiest people and more GPs. Access to GPs is worst where health needs are greatest because these are the most deprived and under-doctored areas. She needs to match funding to need.
3. Good access depends on good management. There’s no reason why the NHS shouldn’t have the best healthcare managers in the world. She should invest in primary care management including finance and HR, within practices and at scale.
4. Of all the new clinical roles in primary clinical pharmacists and pharmacy technicians based in practices are most valuable and these roles should be supported. There is little evidence to show that other new clinical staff can provide support at the scale needed. Undoubtedly there needs to be more investment in practice nurses and District nurses.
5. Continuity of care underpins every aspect of quality, safety and experience in primary are. She should support all measures being promoted by the Royal College of GPs to improve continuity including organisational incentives and public education.
6. She should do everything possible to retain GPs who already have long-term relationships with patients and practices because thousands of them are retiring early, reducing their hours or pursuing other work because the conditions they are working in are too stressful.
7. Satisfaction for patients and GPs is being undermined by a relentless focus on measurement, scrutiny and incentives, so that hours every day are spent collecting data that is of little use to patients or their GPs. She should reduce this as far as possible by following the advice of Don Berwick who the conservative government invited to review quality and safety in the NHS in 2013.
It’s tempting to set targets like seeing patients face to face within 2 weeks but if there are too few staff and the ones that remain are miserable and exhausted then targets like this will only worsen the problem of burnout and GPs leaving. General Practice can be and should be full of joy amidst the suffering and there are still GPs who love their job, but there could be many more, and the government can help with this today.
What too few people appreciate is that complexity is the rule and not the exception in general practice consultations. Few symptoms that patients present with fit with any diagnosis and few problems can be solved by following a protocol or treatment pathway.
Professor of Medicine and Sociology David Armstrong has studied the history of diagnosis and nosology (the classification of disease) “When it [Diagnostic classifications] came to be applied to primary care in the middle of the 20th century, however, it encountered major problems as general practice struggled to marry a classification of disease to the rawness of undifferentiated human illness and distress. Eventually a classification based on the reason the patient consulted emerged to replace that based on pathology defined disease.”
GP records have a ‘Problem list’ on the front page of each patient record, rather than a list of diagnoses. It can include things like, ‘Patient is a carer’ or ‘housebound’ or ‘at risk of diabetes’ as well as symptoms like ‘chronic low back pain’ or ‘fatigue’ alongside diagnostic labels like ‘hypertension’. In the list of past problems might be ‘bereavement, son aged 15, stabbing’, ‘homeless’ (1999-2014), ‘rape’ (2016) – and other significant life events. Problem lists need to be curated by the GP and are a record that depends on what is disclosed and documented. They are always incomplete but are usually better when the patient is cared for by the same clinicians for many years. For psychiatrist Linda Gask who has written memoirs about her near-lifelong depression, her GP was a ‘keeper of her stories’, someone who remembered how she could be, even as they cared for her when she was profoundly unwell.
Epistemologies of General Practice
Epistemologies are types of knowledge and GPs make use of the theory and practice of narrative medicine. In her role as psychiatrist Linda Gask wrote, “For me as a doctor it was the power of those stories and my ability over time to make a difference in how they ended that fulfilled me.” Knowledge of stories is tied up with chronological knowledge of a patient over time. A concept of time, Kairos, not as something linear but as a series of significant moments or episodes is another form of knowledge that comes with continuity of care. The significance of Kairos is that there arise critical moments when a patient may be able to engage with a diagnosis or treatment plan and others when all they need (and can cope with) is caring, kindness and validation. There may be episodes of serious illness when they see a lot of their GP, among occasional brief encounters of little significance.
Other epistemologies are shared by all medical specialties. Knowledge of clinical science (facts), technical and procedural knowledge (how to do things) and administrative /cultural knowledge (how to get things done) need to be integrated with a greater emphasis on technical aspects for surgeons and interventional radiologists for example.
Academic GP Joanna Reeve describes ‘interpretive knowledge and skills’ as being critical for so many of the problems that GPs face. Interpretive skills enable professionals to integrate biomedical, psychosocial, patient and professional accounts of illness in order to make sense of, and so take an active part in managing, their own health problems. They are particularly useful when dealing with chronic mental health problems which is a large part of most GPs work.
Epistemic hierarchies mean that specialist knowledge is valued above generalist knowledge. The specialist opinion trumps that of the generalist, no matter the problem. Generalism and generalist knowledge is low status. Ian McGilchrist has written about how over the last 200 years modern societies have rewarded and promoted specialist – single issue ways of thinking and people with specialist, rather than generalist ways of thinking. The generalist is concerned with the relationships between things while the specialist is more concerned with things themselves (the relata).
The Expert
In his book about the process of becoming an expert, Professor Roger Kneebone describes a journey from apprentice, via journeyman to expert. The expert can improvise with other people, recover when things go wrong, and act safely and confidently where there are no guidelines to follow. They can only do this because they have been learned as apprentice and journeyman to work on their own, to do predictable work, and to use guidelines. So much general practice demands the attributes of the expert because it is steeped in complexity. New GPs who are used to hospital medicine and may still be getting to grips with routine and predictable clinical work, can find the sudden exposure to problems without diagnoses, overwhelming.
Often quoted, Donald Schon advocated for knowledge and skills in reflection practices, so that professionals can appraise the many possible right courses of action that are a hallmark of complex problems.
“In the varied topography of professional practice, there is a high, hard ground where practitioners can make effective use of research-based theory and technique, and there is a swampy lowland where situations are confusing “messes” incapable of technical solution. The difficulty is that the problems of the high ground, however great their technical interest, are often relatively unimportant to clients or to the larger society, while in the swamp are the problems of greatest human concern.”
Education or disposition for complexity.
The rapid introduction of new roles in general practice, in particular Physician Associates (PAs) has raised the question of whether 3 years of training is long enough to develop the attributes of Roger Kneebone’s conception of ‘Expert’ and manage the complexity that typifies general practice. It typically takes 10 years to train a GP; 5 years as an undergraduate, and 5 years postgraduate training. In defending the length of time required to become expert, Kneebone says that “you cannot bake a cake any quicker by turning up the temperature”. The Royal College of GPs which is responsible for postgraduate GP training thinks that it should be longer. The apprentice junior doctor must do repetitive tasks until they can do them in their sleep while being immersed in and becoming a member of the culture of the community they are joining. The journeyman must learn to find their own voice and then learn when to listen to others while embodying the skills they learned as an apprentice until more of their work comes naturally. Some GP trainees never seem to get very far towards his conception of the expert who is comfortable with uncertainty and complexity, while some seem to take to it naturally very quickly, as do some PAs. You may not be able to bake a cake quicker, but some ingredients are better suited to cakes than others. Education may be necessary, but is, at least in its present form, not sufficient for some people to become an Expert Generalist. For one thing, medicine is taught as though every symptom conceals a diagnosis and the job of the doctor is to diagnose the disease and prescribe the correct treatment. The failure to acknowledge that most symptoms are unrelated to any disease and may yet persist for life, is a clinical and moral failure of medical education. It is a major reason for dissatisfaction among patients and professionals. Clearly doctors need to know when their patients’ symptoms do signify a disease that needs treating. But its far from the only skill they need and especially so in General Practice. Education could be better, but even as it is, some people are much better at handling the ‘swampy lowlands’ of general practice than others.
Selecting for disposition
We hope that people with the right attitudes and attributes will find their way into the professions to which they are suited. There is some evidence that a low tolerance of uncertainty is more prevalent among orthopaedic and urological surgeons than among psychiatrists and GPs but we do no more than hope that people able to deal with complexity and uncertainty will find their way to general practice. You cannot be a generalist without being an expert, but expert generalists need disposition at least as much as education. They also need a community of practice, and organisations that recognise their expertise, with high levels of trust in which they are valued and can experiment and learn, in which relationships are encouraged and facilitated. This way they can work effectively with patients and the ‘rawness of undifferentiated illness and distress’.
How does a busy GP provide a safe presence for patients who are vulnerable, and afraid? Is it possible to train oneself to provide whole-hearted attention with good intention 30 times a day or more in the NHS?
In this essay, first published in the Jounal of the British Holistic Medical association, I define therapeutic presence and explain how I have been using the Wim Hof Method to help remain present and grounded in my clinical practice, in order to help patients feel safe and heard. https://bhma.org/
In The Sleeping Beauties, neurologist Suzanne O’Sullivan describes a fascinating, but rare phenomenon which she is perhaps best described as Mass Psychogenic Illness in which many people from a group with shared social experiences experience similar Functional Neurological symptoms at the same time. Lay, media and medical explanations come into conflict, in particular when doctors with vested interests get involved. In spite of how uncommon MPI is, functional neurological symptoms are among the commonest problems that patients present with to GPs and neurologists and there are some lessons, some questions and some problems raised by her account.
The broad spectrum of Functional Neurological Disorders (FND) ranging from dissociative disorders like depersonalisation and derealisation to non-epileptic seizures and the overlap with conditions like POTS, IBS, chronic fatigue, chronic pain and mood disorders, inflammatory and autoimmune disorders makes diagnosis difficult and it is frequently delayed or never made. O’Sullivan includes a case of a young woman who has this constellation of problems, the only non-MPI case in the book and one that she found particularly challenging since she was her doctor, unlike the MPI cases she investigated as a journalist. The hardest part about looking after patients with FND is the relationships between the patients and the doctors. This case will be familiar to most GPs and neurologists and in it lies the most important lesson: key to a good outcome is a therapeutic alliance in which there is sufficient shared understanding and trust for a basis on which healing can occur. Given the healing role of the community which might include a multidisciplinary team, family, friends, teachers, social workers, employers etc. sufficient shared understanding can be impossible to achieve, and the prognosis for FND can be very poor, especially in our modern, fragmented, individualistic society. And as she notes, but could have emphasised more, doctors hold most of the power, responsibility and blame for creating conflict by imposing their own ideas – what Fricker and Cavel call Epistemic Injustice – the imposition of a medical interpretation and refusal to respect any other. The confidence in Western Medicine’s ability to provide a cure for all ills, or our tendency to dismiss things as ‘untreatable’ or ‘treatment resistant’ is another symptom of our arrogance. It’s interesting by contrast that she discovers that shamanic treatments are ‘largely successful’ among the Nicaraguan patients she visits which suggests that a community approach to the understanding and healing of these kinds of disorders could point towards what ails us as a society and that Western Medicine is only one type of medicine among others and progress might require us to look at other traditions. It also points to the power and politics within Western medicine: we use the term biopsychosocial which implies a hierarchy in which the BIO overshadows the psychological and the social is the final consideration. It is also conceived as additive – Bio+psycho+social rather than ecological – an imbalance between constantly interacting parts of a biome which includes safety, security, human relationships, relationships with the natural world, clean air, nutritious food, healthy amounts of acute inflammation from regular exercise and more. The widening gaps between healthcare professionals and their patients due to specialisation and the collapse of relational continuity means we are less able than ever before to integrate historical and social perspectives.
Unfortunately we’re in a situation of catastrophic climate change, the collapse of biodiversity, alienation from the natural world, the Covid pandemic, worsening pollution, rising inequity, highly processed foods, rigid and competitive education systems and neoliberal corporate capitalism, so it is very hard to be well and it’s no surprise that the numbers of patients presenting with FNS and all the associated autoimmune/ inflammatory disorders are on the rise and doctors are overwhelmed.
On a final note, O’Sullivan is at pains to emphasise that MPI/ FNDisorders are NOT caused by trauma and on this I fundamentally disagree. Firstly FND may in some bars be the presenting symptoms of present and ongoing abuse, just as women who are being abused are more likely to come to tell their GP about pelvic pain than the violence they’re experiencing. I can see why she is at pains to do play down trauma almost too three point of dismissal because when asked about ACEs (Adverse Childhood Experiences) many people with MPI/FND will say that they didn’t have any. And also the experience of many people is that admitting to a history of Trauma leads to their problems being dismissed as psychological or even worse they are labelled as having a ‘personality disorder’ at which point they are repeatedly re-traumatised by medical systems and professionals. Bringing up ACEs risks parents or others being blamed and may lead to huge disruption to families. Trauma, especially in MPI occurs to communities, and Joy DeGruy had written about Post-traumatic Slave Syndrome. My experience is different from O’Sullivans because I’ve been in the same practice with high levels of continuity of care for over 20 years so my view is ecological – I see historical, intergenerational, cultural, community, environmental factors interacting and I see constellations of symptoms and diagnostic labels come and go – my patient encounters may be ultra-brief, but over decades they become ultra-long. I am also learning how to provide presence – a safe, holding space where we can acknowledge trauma – which often stems form never having been held in a safe space – not just the experience of abuse. Providing presence and a safe space means the doctor getting their ego, interpretations, ideas, assumptions, emotions and other baggage out of the way, being attuned to neuroception (recognising how their nervous system responds to the presence of another) and being open to the experience of being attuned and affiliated however painful that may be. And while I know many people who can do this naturally, we are a very long way from teaching or promoting it in Western Medicine. But very often we don’t know what happened and we should not go digging, after all, trauma – as Gabor Mate explains it, “is not what happens to your body, it’s what happens inside your body”
Anyone suffering with chronic pain or treating or caring for someone with chronic pain will be relieved to discover that MINDSET isn’t a just a state of mind, but an acronym for 7 steps to help with recovery. It is the work of Dr Deepak Ravindran, a pain specialist whose journey alongside thousands of patients with chronic pain has given him the confidence to wrap what he has learned into a practical and largely accessible 7 steps for taking control and overcoming chronic pain.
MINDSET stands for: Medication, Interventions, Neuroscience (and stress response), Diet, Sleep, Exercise (and movement) and Therapies (of the mind and body).
The Pain-Free Mindset is a workbook filled with suggestions for making progress in every one of the 7 steps which can be DIY (Do It Yourself), DWY (Done With You aka ‘supported self-management’) or less frequently DFN (Done For You). Reading the book isn’t going to relieve your pain, but returning to it over and again and working on the 7 steps will undoubtably help you make progress. Patients and clinicians frequently feel stuck when trying to cope with chronic pain and the beauty of this book is that you can either work at the area you’re stuck with or focus on another step that’s been overlooked or is more easily achievable. Sceptical readers might quibble at the alternative therapies included but would do well to remember they’re included as part of an overall package of care and not promoted as cures.
One thing that perpetuates chronic pain is inconsistent and unhelpful advice from professionals and this book includes several accounts of patients who were poorly advised by doctors promising a simple explanation or solution to their chronic pain. Much as we might want pain to be a simple matter or for a pill or a procedure to make our lives less painful, the truth is that coping with pain requires attention to every aspect of our lives – or all 7 MINDSET steps.
What stands out by omission is that pain is a social justice issue – social exclusion by poverty, gender, race, trauma, disability, imprisonment etc. vastly increase your risk of suffering with chronic pain. The more ways in which people are disadvantaged the more likely they are to suffer pain and the harder it will be for them to follow the 7 steps. My own (White, middle-class, professional) lifestyle measures up pretty well to Dr Ravindran’s 7 steps, and I’m sure his does as well. It’s a healthy lifestyle for everyone to aspire to, not just people with chronic pain. You might as well say, ‘Don’t be poor, have supportive friends, have time to cook and live near safe, green spaces.’ I work in an urban practice with high levels of poor housing, airborne pollution, food-bank dependence and social isolation where chronic pain is as prevalent as asthma and diabetes. People’s choices are constrained by their circumstances.
I’m not nihilistic about chronic pain, far from it, and both Dr Ravindran and I have over 30 combined years of working with the same patients and have seen enough of them improve to know that people do get better, even in deprived areas. But very often what’s required is a change in circumstances beyond the control of the doctor or the patient – for example, a violent partner leaves or they start a satisfying job with a living wage.
That said, if you’re feeling ‘stuck’ with chronic pain and want a better understanding of how mind and body interact to determine how we experience pain and what we can do about it, then this is a great book that is full of ideas for progress that I have no hesitation in recommending to patients and it will be their feedback that I’m especially interested to hear.
I very rarely come across someone with chronic pain who isn’t suffering from trauma – not the catastrophic injury kind of trauma, but the kind of development under stress kind that leads to the trauma world in later life.
Making the link between chronic pain and trauma, as I often do, divides audience between those for whom it validates their experiences and those for whom it invalidates the all-too-visceral nature of their suffering.
The validation / invalidation divide is often so powerful that any attempt at paddling backwards to explain what I mean often further alienates people who have previously experienced the pain of invalidation.
Professor Paul Dieppe, a retired rheumatologist who has become increasingly interested in pain, suffering and healing, explained to me that invalidation is a more powerful force for harm than validation is a force for good and my experience has taught me that this is true. It is very hard to regain trust from someone who has experienced invalidation by your words or behaviour.
Trauma informed care is sometimes assumed to mean clinical practice in which past traumatic experiences are used to explain present symptoms. This is untrue and an unfortunate misrepresentation – unfortunate because recounting past experiences can be traumatic for patients and clinicians; unfortunate because the links are long and complex and far from being fully understood; unfortunate because it can lead to the assumption that people with a history of trauma need psychotherapy but not immunotherapy; unfortunate because of the profound shame and stigma associated with past trauma; unfortunate because trauma informed care can and already is, radically transforming care for the better.
A useful definition of Trauma Informed Care is the 4 Rs.
Realises what we mean by complex trauma and toxic stress; how prevalent traumatic experiences are and who is most at risk (women, people living in poverty, people with disabilties, ethnic minorities and other marginalised and stigmatised groups)
Recognises the signs and symptoms of the trauma world – the hyper/hypo arousal, toxic shame, dissociative symptoms and coping strategies used by those who are affected
Responds in ways that prioritise safety and trust, show empathy and understanding and enhance the potential for healing
Resists any ways of behaving that might re-traumatise people
It’s worth noting that trauma informed care is an organisational and an individual approach to working and not something that you do with certain patients. It’s a way of working with everyone.
So why bring up Chronic Pain?
I’ve recently looked through records of patients registered at my practice to identify those that are suffering with chronic pain. First I looked everyone diagnosed with chronic pain and associated problems like Fibromyalgia and Chronic Regional Pain Syndrome. Next I looked at all the notes belonging to patients prescribed opiates, Gabapentinoids and tricyclics – the most commonly used drugs for chronic pain. I went through the notes to see whether they were taking the medication for chronic pain. In total I identified nearly 550 patients accounting for about 4% of the practice – making Chronic Pain the fifth most prevalent long-term-condition after Hypertension, Depression, Asthma and Diabetes. On average patients with Chronic Pain contacted the practice 33 times per year, 3 times more than average. I asked patients and colleagues what to include in an annual review and I am trialling an annual review lasting 20-30 minutes with their usual GP.
The new NICE draft guidance for chronic pain has a definition of chronic primary pain as ‘characterised by disability or emotional distress not better accounted for by another diagnosis of chronic pain.’ In practice it seems to make little difference whether someone’s chronic low back pain can or cannot be explained by osteoarthritic changes on an X-ray or disc-degeneration on an MRI scan. Whether there is another diagnosis to account for the pain makes little difference to the degree to which the pain can be tolerated or is unbearable. A pragmatic definition that I used in defining Chronic Pain for my patients was, ‘Pain of any cause that is hard to bear and is the primary reason for repeated consultations’. Conditions like arthritis, fibromyalgia, chronic pelvic pain (including endometriosis) and irritable bowel syndrome may be included, so long as pain is the primary issue for repeated consultations.
Pain and the Trauma World
The Trauma World is a description of the problems people live with as a result of growing up under conditions in which their threat response, a set of protective, primitive reflexes is chronically, repeatedly or severely activated. Developing bodies and the biological systems within are remarkably resilient, but under sufficient stress, especially at certain critical times for example in utero or infancy, they are susceptible to lasting effects. If protective, buffering factors like maternal bonding and emotional intimacy are absent then less severe stressors may have lasting impacts. Immune/ autoimmune, neurological, gastrointestinal, cardiovascular and other symptoms are activated by the stress response – that results in symptoms including palpitations, rapid breathing, vasodilatation and sweating, fearfulness, dyspepsia, nausea, the urge to urinate and defecate, and if severe can lead to collapse or fainting, blackouts, seizures or other dissociative symptoms. Growing up in a situation of helplessness, where fight or flight is impossible and there is nowhere safe to go for comfort or protection leads to this biological over-activation being internalised, only to cause problems later on, sometimes decades later. The shame and stigma, disbelief and invalidation that often accompanies the these stressful situations, mean that even as time goes by it may very difficult to talk about what has happened, and this is as true for childhood neglect as it is for domestic violence. More often than not, it is sufficient to acknowledge that stuff happened without trying to catalogue the details.
It follows from this that everyone experiences some degree of stress growing up and some traumatic symptoms later on, but there is a dose-response whereby more severe threats and fewer protective factors lead to more problems in later life. This is why many patients present with multiple related symptoms, for example – chronic dyspepsia with irritable bowel syndrome, chronic anxiety, urinary incontinence, and autoimmune diseases like SLE or Psoriasis in addition to chronic pain. Patients with chronic pain alone may have been fortunate enough to have suffered less developmental adversity, but very few of our patients with chronic pain, suffer only from chronic pain.
To return to the 4Rs of trauma informed care in relation to patients with chronic pain.
we
Recognise that the burden of chronic pain is unevenly distributed – women, people living in poverty, people with disabilties, ethnic minorities and other marginalised and stigmatised groups are disproportionately affected.
Realise that chronic pain rarely occurs without other manifestations of the trauma world including autonomic dysfunction, chronic anxiety, gastrointestinal and urinary symptoms, autoimmune diseases, dissociative disorders and shame.
Respond in ways that seek to provide kindness where there has been cruelty, validation where there has been disbelief, vindication where there has been blame and continuity of care where there has been rejection and a lack of commitment
Resist re-traumatising patterns of behaviour including invalidation and blame
I have learned the hard way that patients don’t want me to explain pain or trauma. I tried and they told my in all sorts of ways to stop. It’s their pain and their trauma, my job is to understand it better. The desire to ‘painsplain’ is born out of insecurity and wanting to reassure them that I know what I’m talking about. I’ve learned the importance of ‘asking the questions whose answers need to be listened to’ and that ’empathy is always poised between gift and invasion’ (thank you Leslie Jamieson). I need to keep remembering that patients will forget most of what I say, but rarely ever forget how I make them feel.
Trauma Informed Care is a journey, not a destination. We’re trying our best, and although there are many inspiring pioneers, these are uncharted waters and only by working together will patients and clinicians find our way.
Social hierarchy in medicine dictates that doctors diagnose and treat while caring is delegated downwards as far as possible, from nurses to healthcare assistants, home carers and millions of unpaid family, friends and volunteers. Caring is low status work, no matter how high its moral status or how earnestly it is invoked in political rhetoric. We want to be seen as caring without having to do the actual work of caring, because actual, physical caring involves getting your hands dirty, and being exposed to things we would far rather avoid.
Madeleine Bunting quotes B.J.Miller a Californian Palliative care doctor, “Palliative care is that art of not running away” but in my experience, remaining present at the end of life is often easier than handling incontinence, or infected wounds, or caring for older people with severe dementia, or children with serious disabilities , caring for addicts or people affected by suicide and the aftermath of abuse, psychosis and more. Faced with foul smells, hostile behaviour and intolerable suffering the natural impulse is to run away and yet there are people who remain present and provide care.
The social determinants of suffering mean that the more you are deprived of money, social networks, education and/or a nurturing environment at the start of life, the more likely you are to need care. The Inverse Care Law – first described by GP Dr Julian Tudor Hart in 1971 – shows that the provision of healthcare is inversely proportionate to the ned for it and these disparities are wider the more that market mechanisms are used to drive distribution. As we move from a recession bought on by the financial crash in 2008 to another bought on by Coronavirus in 2020 – we are experiencing ever-tightening public funding for care and even wider inequalities in the need for and receipt of care.
Labours of Love is a call to action. The Philosopher Michael Sandel argued that we have moved from a free-marked economy to a free-market society, bringing in the incentives and morals of free markets into the social world where they do not belong. We need to bring the incentives and morals of care and caregiving into society. To do this we need to learn the Art of Not Running Away.
When we have been able to afford it, we have paid for others to deal with work which bores, frightens or disgusts us. Different kinds of caring are more tolerable than others. In popular culture there are no shortages of images of healthcare professionals and others caring for people who are wounded or dying, but very few involving the care for people with skin diseases, neurological diseases, mental illnesses, or learning disabilities. There are few images that depict the horror. Care is depicted as something calm and kind. What is missing is the emotional labour, the moral agony of having to do too much for too many in too little time, without support while repeatedly suffering the guilt of having done too little in too much of a hurry.
The people who provide care and the people they care for are out of sight and out of mind. Many carers are so preoccupied with caring that they barely have time to spend with their colleagues. As Bunting shows, this isolation makes it almost impossible for them to associate and organise to do anything about the rights of carers. They are frequently exploited by employers and the state and right now are among those at highest risk of infection from coronavirus.
A lot of a general practitioner (GP) work involves caring. The motto of the Royal College of General Practitioners is ‘Cum Scientia Caritas’, which can be translated, ‘With science, caring’. Very little is written about the caring aspect of the job, compared to the science. I would estimate that over 50% of my consultations involve little more than caring. Over the course of the last 20 years as a GP I am confident in saying that caring is far from simple, ‘unskilled’ work. A friend (another GP) has recently given up his third partnership and admitted that for the first time in years he can sleep without worrying about patients at night. For years he had argued that GPs needed longer training to learn the breath of medical conditions they needed to manage, but in the end I think it is not the knowledge that GPs struggle with, but the relationships. The GP and author Ian Williams said that he had to move on every 5 years to escape the complex relationships with patients that inevitably developed and his graphic novels are creative, sometimes cathartic attempts to work through some of these relationships. In workshops that I have been running for GPs and GP trainees about Trauma Informed Care I say that without continuity of care it is impossible to provide effective care for patients who have experienced trauma – at which point, usually one or more GPs says that continuity is impossible where they work – and I can see, by the way they say this, that they are suffering. In 1959 Isabel Menzies Lyth was asked to carry out an investigation into an NHS teaching hospital in crisis. Senior nurses felt the service was at the point of breakdown and one third of nursing students were giving up their studies. She noted,
Nurses face the reality of suffering and death as few lay people do. Their work involves carrying out tasks, which, by ordinary standards, are distasteful, disgusting and frightening. The work arouses strong and conflicting feelings: pity, compassion and love; guilt and anxiety; hatred and resentment of the patients who arouse these feelings; envy of the care they receive. The intensity and complexity of the nurse’s anxieties are to be attributed primarily to the peculiar capacity of the objective features of the work to stimulate afresh these early situations and their accompanying emotions.
Recognising the fact that the emotional labour of care was so hard for the students, senior nurses and management decided to break apart possibilities for continuity of care. The consequence was that the students became more distressed. People who want to care, need to be given the opportunity to develop caring relationships and the resources to do their work properly.
Reciprocity
Reciprocity is a theme that recurs frequently in Labours of love. In caring, carers are constantly attentive to the different ways that the one they are caring for is responding, adjusting what they say, how they present themselves and how they touch. Care is a multi-sensory experience, which is why, even during a pandemic, the majority of my face to face consultations are for mental health. Caring is a creative act, improvising in harmony with those we’re caring for, getting into a caring groove. It’s enormously satisfying to accompany someone back from a panic attack or a psychotic or dissociative episode. Our natural propensity for empathy means we share in the pain and the relief. It feels good to care.
Care can quite frequently involve pain as well as pleasure. It can be the physical pain of dressing leg ulcers, or performing dental surgery, but in my work, it is often psychological or emotional pain. In providing care for people who have experienced trauma relating to abuse, trust is hard-won and consultations, at least to start with, are quite frequently challenging as patients and doctors push one another to work out where our limits lie and how much we can both be trusted and whether our care is genuine. The path of least resistance may be to whatever is necessary to keep consultations short. I have a picture on the wall of my consulting room, above where patients sit, that says, ‘Remain Kind’. I would like another that says, ‘Stay Present’. It is one of the most important things I can do when confronted by someone who is angry, anxious, paranoid, and frightened. Consultations and thank-you cards begin, ‘Thank you for putting up with me … ‘ an acknowledgement that caring relationships are hard at times.
Meaningful care work with patients like this delivers delayed gratification. There is pain before gain. As the possibility for continuity of care gradually fades away, I worry that General Practice will become less caring. For Arthur Frank, medical sociologist and anthropologist, ‘The structured disruption of continuity of relational care is more than an organisational problem; it is a moral failure of health care, deforming who patients and clinicians can be to and for each other.’
Touch
Not long ago I was watching a GP trainee examine a woman to feel for a breast lump. The trainee put on a pair of surgical gloves before examining her. Afterwards I invited the women to give some feedback. I asked her what she thought about whether doctors should wear gloves during a physical examination like this. She said that she worried that the doctor would be less likely to feel a small lump. She said she would have been more reassured without the gloves. Touch can be both instrumental and affective at the same time. The instrumental touch is informed by knowledge of breast lumps and anatomy; the affective touch is confident, kind and reassuring. In another situation I was watching a medical student perform an abdominal examination. The patient took her hand and pressed it down on her abdomen instructing her – “You need to feel deeper than that”. This act of instruction was also instrumental and affective. If we are to find what we are looking for and at the same time reassure patients we need to be firm. I don’t tend to hug my patients and I’m not really comfortable with touching arms, hands or shoulders in acts of comfort. But patients in mental distress present with physical symptoms all the time, inviting a physical examination which is an act of communication. They invite a clinical examination by locating pain in their bodies. Bodies can give away what may be too painful to discuss while hands can provide reassurance that cannot be put into words. A colorectal nurse specialist recently told me that nearly 50% of her adult patients with chronic constipation were abused as children, “They are shut off from the waist down” she said. Many of them also complain of numbness and weakness below the waist. We need to be aware of how trauma affects patients – as one survivor of sexual abuse writes in an open letter to her doctor,
You may be the first person we allow to touch our bodies after they have been desecrated by another’s hands. It is terrifying, shameful, and a very painful experience. In those moments, some of our most vulnerable, we need your patience. We need kind and honest words in a gentle tone, and we need a slow and understanding touch that is safe for us to say no to.
Caring requires disposition and labour. Our dispositions are shaped by our experiences of being cared for. Care is hard labour. Part of the high moral status of caring comes from a recognition that the work, and the conditions are harsh and risky. This hard work requires resources including time and support. People who are disposed to care but lack the resources will burn out because of the repeated experience of not being to care to the standards they have set themselves.
Excellent, caring professionals are giving up caregiving roles every day. Burned out doctors and nurses are withdrawing from work that is tied up in caring relationships. They are moving to organisational, administrative, signposting roles, facilitated by the rapid shift away from face to face consulting. We risk squandering the good will and natural inclination of millions of caring people by expecting them to care with little more than their own kindness to sustain them. If we want to raise the status of care and create a more caring society, we need to acknowledge and materially support the Labour of Love.
Consider the following statements: “Dr Brown is treating my depression” and “I am seeing Dr Brown for my depression”
Illness commodified becomes something separate from the person – this thing we call ‘my depression’ implies that it is not me that is depressed, but a thing apart from ‘me’. We (Dr Brown and I) can then work out a treatment plan for this thing we call depression – Sertraline, CBT, some graded exercise and less alcohol.
I’ve been wondering what it means to be seeing Dr Brown for my depression.
I have had therapists. And I wouldn’t say that she’s my therapist. I was intrigued to discover that Sigmund Freud did not consider himself a therapist. In fact he deliberately chose not describe his work as psycho-therapy. The one time he visited the United States, it was at the time that the American Medical Association ruled that only qualified doctors could practice psychoanalysis and he feared that instead of exploring patients’ psyche they would attempt to diagnose and cure them. He never visited the US again.
Let’s not pretend for a moment that I wouldn’t be glad of a cure and to be rid of the depression that’s ruining my life and my relationships (or what’s left of them). I’ve got nothing against cures. I’m not so sure that I’m so interested in being diagnosed any more. Being told that I’m suffering with ‘depression’ or ‘anxiety’ or ‘panic attacks’ or that I have ‘chronic pain’ or a ‘borderline personality disorder’ hasn’t been especially helpful. Most diagnoses are tautologies – I’m depressed and anxious so I’m suffering from depression and anxiety. Being told that I’ve got a personality disorder was helpful only in so far as it made me question the whole diagnostic process. Does a diagnosis help me make sense of how I feel? Does it help me access the help I need to get better? Are diagnoses objective truths or historical artifacts?
I’ve been depressed for so long now that I wonder what would be left without my depression, but perhaps I’d settle for there just being less of it. Freud said something about wanting to help people shift from having a pathological, debilitating depression to an ordinary depression. Perhaps that would do.
Depression isn’t something I can fight. I’ve heard of people with cancer object to fighting talk and war metaphors; war on cancer, fighting back, being strong, winning the fight or giving up the fight, or being defeated by cancer. I’ve seen people almost killed by friendly fire in battles against cancer – hairless, bruised and bleeding, sepsis, diarrhoea and vomiting, dehydration and renal failure. And I’ve seen the same damage done in battles against depression – rendered fat, impotent, diabetic and zombiefied by the drugs, re-traumatised by therapy, brutalised by confinement. I think the problems are inherent in all types of healthcare, not just mental health.
The more I think about it, I cannot separate my depression from me – how ever much I’d like to. Perhaps there was a time, at the beginning. Maybe there is another me: less antisocial, less self-loathing, more worthwhile underneath this fog of depression. Waiting to come up for air. But now I’m not so sure. The depression and me have become one.
Validation
I do remember at some point thinking, ‘she believes me, she actually believes me!’. I don’t remember exactly when that was, but it was sometime in the beginning of 2018. The hard part was trusting her enough to believe her when she said that she believed me. Practically my whole life I’ve trusted people; from when I was a kid or too naïve or too vulnerable and they’ve taken advantage of me, until I couldn’t trust anyone any more. And this is what it has been like with doctors. You’re vulnerable, afraid, trying to get help, and they expect you to trust them. And I’m thinking, ‘yeah, right, where have I heard that before?’ And I can tell you exactly where I heard it before. And I can tell by their body language and the way they say it whether or not they mean it. And nine times out of ten they don’t. They’re saying it to get you to take the pills or stay in hospital, or sign the form or whatever.
It wasn’t easy to trust Dr Brown to begin with. There wasn’t a particular moment when I went from not trusting to trusting, but there was a time when I went from not trusting to trusting her enough.
Even now I worry about how much I can say. How much she can handle. I have to make a judgement about how busy or stressed she seems, I worry that she’s going to get fed up with me calling or won’t be able to handle how messed up I am. I remember an online group where I was been warned not to tell her about my fits I was having. The other people in the group said that’s a sure way your doctor will think you’re mad because they’re not real epileptic seizures. I did tell her one time, but only when she asked if I ever had them and we talked about a film she’d seen about people who had been abused that suffered from dissociative seizures afterwards. She seemed genuinely curious and not at all judgmental.
Vindication
If there’s a key to our relationship, I think that it’s the fact that she’s not judgmental, or rather she is judgmental but not in the way I’m used to. What I’m used to is being blamed – for everything; for everything I do and for everything about me. That’s how it’s been my whole life. I was born wrong, a mistake from conception. I’ve got personality disorders to prove it. “you know what?” she says, “It’s not your fault”. If I’m in the right frame of mind I want to give her a hug when she says that, but mostly I want to scream, “How. Do. You. Know? What can you possibly know about me that I don’t know?” There are things I’ve done and said and thought that she’ll never know, even if there are things she already knows about me that nobody else knows. There are thoughts that terrorise me in my nightmares and flashbacks that I’ve spent years trying to blank out with sex and drugs and booze and cutting and bingeing and the rest.
Carl Rogers came up with this idea of Unconditional Positive Regard – which means seeing the good in the other person. It’s like not being judged, so that no matter what you say or do, like when you’ve fallen off the wagon and gone on a bender we can agree that wasn’t such a good thing to do, but it doesn’t change who I am. It doesn’t alter the fact that underneath she still thinks I’m worth looking after again, and again and every other time I screw up. That’s why it’s unconditional and it’s positive because she thinks I’m worth it, and the ‘regard’ bit? Well that’s like presence.
Presence
There are times when I have screamed at Dr Brown. Perhaps not at full volume, but I’ve lost it. I know what Hilary Mantel meant when she said, The sufferer is in a state of high alertness and of anger looking for a cause. What strikes me is that (in my case anyway) anger comes before the pain: a wash of strong, predictive, irritation emotion that I don’t feel at any other time. What I remember is how calm my GP was. I need a doctor who can handle my pain, my anger and my losing it from time to time. Someone who doesn’t recoil and try to get rid of me with another prescription or a referral. Someone who can bear the fact that they don’t know the answer and they can’t fix me. Someone who can bear to be with me when they don’t know what to say and not fiddle irritatingly with their computer or launch into a long unsolicited explanation or piece of advice. I think that asking your GP to be present shouldn’t be too much to ask, but God knows it’s a rare and beautiful thing, because presence is what I need when I’m unbearable. That’s when I’ve been sectioned, sedated and restrained. It doesn’t make so much sense at the time, but I can see it now, thanks to Dr Brown. The times when I’ve hated her most are when she’s failed at that. When presence is what I needed, and she wasn’t there for me. The point is that it’s when I’m hardest to be around that I need her to be present and that’s what brings me back to earth.
The Good Enough Doctor
Donald Winnacot wrote about the Good Enough Mother in 1953. He was a jobbing paediatrician who saw thousands of mothers and babies as well as being a psychoanalist. He came to realise that babies and young children benefit when their mothers failed them in manageable ways. By these small failures of care-giving, these cracks in their mothers’ carapace of infallibility they realised that they could cope without them after all but that it wasn’t a total catastrophe if sometimes she wasn’t there. I know a lot of Dr Brown’s other patients. I can imagine what it’s like listening to them all day. No wonder she’s sometimes not so present after twelve hours at work. It’s good too, to realise that she’s a normal person which gives me hope that you don’t need to be a saint to put up with me.
Perhaps more simply, what I get from my GP is acceptance and commitment. Put like that it sounds a bit like I’ve got to put up with how I feel and with what I’ve got. Which is a bit disappointing. After all most people go to the doctor to get a cure or at least a bit of symptom relief. When I started seeing her that’s definitely what I was looking for. All my friends were telling me to go back and demand that if she couldn’t tell me what was wrong or fix my pain she should refer me to someone who could. I was hearing all these stories about people who got sick or died because their GPs didn’t refer them in time. I’m pretty sure she was offended, her professional pride dented. I thought she was saying it must be in my head because the blood tests didn’t show up anything. She even used a phrase later on – something about changing role from ‘tour-guide’ to ‘travel agent’ from care-giver to care-navigator. But I didn’t see it like that. Why couldn’t she be both? Why give up on caring for someone just because you’re referring them to a specialist? Why stop being there for someone just because someone else is there as well? She’s in my life for maybe 10 minutes a month these days and even at the height of my troubles, barely 20 minutes a week. Sometimes I think she needs to remember that. “There are too many of us for the likes of you” I told her one day. ‘You might think it’s all down to you, but it’s not’.
I don’t know how she does it sometimes. Working around here there’s a lot of mental illness, lots of drugs and alcohol, lots of arguing and fighting. Lots of people worse off than me. I’ve seen the receptionists get it in the neck something terrible too. What they have to put up with, it’s a wonder they haven’t chucked half the patients off the list. But I hope they’re getting looked after too, all of them. You can’t look after other people if you’re not being looked after yourself. If there’s one thing she’s taught me it’s that. I’ve always found that the hardest thing. And I worry it’s the same for her too.
Every year millions of patients submit online feedback to the NHS via NHS Friends and Family, NHS Choices, Care Opinion, Google, Twitter, I Want Great Care etc. The vast majority is never read or replied to, let alone acted on. Most of it is a massive waste of time. There is no consensus on either how best to collect feedback or how it should be used. This problem probably stems from the fact that it is a ‘complex intervention’ which means that it is impossible to predetermine the outcomes. But we are where we are, which is a muddle caused by being stuck on trying to figure out what it’s for and how to do it.
The separation of means and ends is the subject of a useful paper on the ethics of healthcare improvement. Ethical ‘means’ require that feedback is representative, unbiased and confidential if those giving it wish it to be. The process of giving and administrating feedback should not be too costly or burdensome in time or resources. There should be consent before giving and being given feedback but patients are pressured into giving it and clinicians are forced to collect it, publish it and submit it in their appraisals. Rarely are these basic ethical principles satisfied.
Ethical ends or outcomes include avoiding harm. Negative feedback can prejudice future care for the patient and can be upsetting, even, in exceptional cases, to the point of suicide for the recipient. Every doctor I know has lost sleep over negative feedback, but few have ever celebrated or even slept better after positive feedback. It is impossible to measure the amount of positive feedback required to balance a single piece of negative feedback. Some feedback is moderated by NHS Choices and Care Opinion for example, but even defamatory feedback left on Google or other sites can be harmful, hurtful and impossible to remove. Another ethical outcome we would hope for is that feedback results in benefits for patients, clinicians or services. But there is no consensus on what patient feedback is for, never mind what it should achieve. Some people view it as a quality improvement tool – for which there is no compelling evidence. In this respect it is hampered by inappropriate means – it is usually unrepresentative and non-specific. Others view it as a recruitment tool – like a hotel or restaurant review; in these cases the means are often manipulated and providers solicit feedback from patients who have already expressed satisfaction.
But what do patients think it is for or want it to be for? In a small study of patients who used online feedback the general view was that they wanted a dialogue about their experiences with service providers – engagement with feedback was the outcome; the means were the ends.
In the last few years, I have been a patient on several occasions on account of being accident prone and breaking bones or knocking myself out. I almost always give feedback. I see giving feedback from the ethical perspective of duty. I have never had any useful engagement. I have had my concerns dismissed and ignored. Recently after a poor experience I gave my feedback by Twitter. I was upset and in pain. I called the people in the department ‘idiots’ which looking back from my present calm, well fed, less pained perspective, was inappropriate, but at the time was a fair measure of how I felt. As a healthcare provider, encouraging feedback by social media, you have got to expect people to vent their frustrations. What follows from that is that you have to be able to respond- promptly, with an apology. I wanted the same as the patients in the study referenced above. But I didn’t get it; they did not even say sorry.
There are some good people doing good things (thank you James Munro of Care Opinion and Lee Morgan of NHS Choices). But mostly the ethics, like the feedback, is missing. And feedback is failing patients and clinicians alike.
Conversations about care: interview study with patients and their family members to explore their perspectives on and experiences with online feedback about NHS services https://www.ncbi.nlm.nih.gov/books/NBK549387/
“Change means growth and growth can be painful. But we sharpen self-definition by exposing the self in work and struggle together with those we define as different from ourselves, although sharing the same goals.”
Audre Lorde
I grew up in Kent, in South East England in the 1970s and 80s. I didn’t meet anyone who wasn’t white until I was about 12 or 13 years old. My only exposure to black people was in National Geographic magazines where they were an exotic curiosity or occasionally on television where I remember children’s TV Play School presenter Floella Benjamin and decathlete Daley Thompson. It was normal when I was growing up to hear adults refer to black people as ‘Wogs’ or ‘Coons’. I remember coming to London once with my dad to watch a Rugby match and seeing a Black man on the underground and remember pointing to his stereo and saying to my dad, “look at that man’s ‘wog-box’” and my dad being cross with me and pushing me back onto the train. I felt betrayed because this is what he used to say and now it seemed that there was something wrong with it. I also remember teasing a black boy at Judo club with racist names. I must have been about 6 or 7 years old. I remember him being upset and attacking me, but I don’t remember anyone telling me off or racism ever being mentioned. I don’t think I even thought about racism until I was a teenager.
The death of George Floyd was an inflection point, forcing many of us to confront the question, “What should we be doing about racism?”
Robin Di’Angelo’s answer to this question is, “What has enabled you, as a white person, to live your entire life without having to answer that question before? How were you able to ignore or avoid even having to think about it until now?”[1]
She argues that the problem is not one of racist people behaving badly in a tolerant culture, but a racist culture that conditions people to act and think in racist ways. You need to think and act counter-culturally to overcome racism. As Malcolm X put it, “You can either be racist or anti-racist, there is no space in-between where you can be ‘non-racist’”. Framing racism as a cultural issue makes us all complicit.
So, this month, I ran a session about racism and medicine at work[DG1] . It was set up as a tutorial for two physician associate students and two GP trainees. I also invited our reception manager (a Black man) and a patient (a woman with a Black Caribbean father and a White mother).
Little preparation was required. I told the people coming that the subject of the session (a trainee tutorial) was racism in medicine and that it would last 90 minutes. We found a room that was big enough and well ventilated enough to meet safely in a time of Coronavirus[DG2] . I chose to facilitate the session and explained that we were going to begin with a personal story. The only rule was that in responding to peoples’ stories [DG3] we were only allowed to ask questions about facts, feelings or interpretations, but we were not allowed to offer any opinions or interpretations of our own. While we had called the session ‘Racism in medicine’ we made little mention of medicine. Racism has similarities with illness and disease. Disease is defined by people in authority. You might consider yourself to be suffering, but it is not a disease unless a doctor says it is. Illness is what patients experience: the ways symptoms impact on functioning, relationships and social interactions. To understand a disease, for example Diabetes, you need to know about the pathology and the impact on people’s lives.[2] To understand racism you need to understand facts and figures as well as the everyday experiences of people affected by racism. At our session there were no experts deciding whether something counted as racism. We were there to understand racism as lived experience.
I had not consciously designed the session with the following in mind, but these are some of the things we achieved.
No hierarchies. Nobody in the room claimed to have any greater expertise in racism than anybody else. We were bringing our stories and our skills as listeners.
Epistemic justice. This combines narrative justice and hermeneutic justice. Narrative justice is when accounts that tend to be unheard, ignored or dismissed are invited, listened to, and taken seriously. Hermeneutic justice is when interpretations that tend to be unheard, ignored or dismissed are invited, listened to, and taken seriously.
Bearing witness. Bearing witness to suffering is uncomfortable for the witness. Whenever we listen to stories of racism, we should expect to feel uncomfortable.
No shame. This is not a place for White shame. My story concerned a young child who grew up ignorant. Once I found out what racism was, I changed my behaviour.
Time to think. Tightly structured sessions that are full of activity can stop people thinking deeply because participants are focused on achieving tasks and keeping to time. I did not know where the session would go and wanted to leave time for discussion.
1970s Britain was a great deal more racist than it is today, but the stories the other people in the room shared, revealed that racism is still very present today; in schools, universities, GP surgeries (including our own), the streets of Hackney, medical school, online – everywhere. Di-Angelo was vindicated, racism is systemic. It was an experiential learning session – we acted with humility, curiosity and empathy. The stories are confidential, but one I can share.
For years, one of receptionists has received more complaints than any of the others. The complaints are about her attitude, about being given the wrong information, about being unhelpful, just about everything and anything. We have to apologies and respond to the written complaints and have supported her and given her additional training. In the middle of March this year, we had to close the doors of the practice and patients had to call before coming in. Overnight and without precedent patients stopped coming to the reception desk. Since then she has had no complaints. And she has taken more calls than any of the other receptionists. Since patients stopped seeing her as a Muslim woman with a headscarf they stopped complaining. The sudden cessation of face to face contact at the reception desk was a natural experiment that helped demonstrate one way that racism operates.
In response to the session, Andre our reception manager said,
“I’ve never been asked by a white person about my personal experiences as a black man
I quickly realised that I have supressed feelings about my past/present experiences.
I want to make you understand that we have been conditioned to think that nothing will be done about systemic racism so we just keep calm, carry on and play our position!
This session made me feel very empowered and gained my trust. This enabled me to share my stories with you (as a white man), without fear of judgement &consequence”
Sharon, who came to share a patient perspective said,
“Thank you Dr T for inviting me; some powerful thoughts & thank you Andre for maintaining my faith in my black brothers.
Of course anger, frustration & confusion is paramount when your voice, your history & culture is constantly ignored & ridiculed. Who put the chip on my shoulder…?
Education, Empathy & Respect are a pretty good prescription! Thank you, the more we discuss & learn the less pain to endure.
Years of having to stay quiet & ignore the horrid side of our British History very frustrating! I think our Society as well as the rest of the world finally accept that 400years of slavery simply won’t go away or be forgotten”.
All the practice staff have been buzzing about the session. Other receptionists and clinicians have asked to come to the next session, and I have spoken to other patients about it. For years we have been trying to tackle overt racism – taking action when people are racially abusive, but now we have found a way to do something about systemic racism. The session cannot stand alone, and it must be repeated regularly. But it is an important start.
[1] DiAngeloo R. White Fragility: Why it’s so hard for White people to talk about race. Beacon Press 2018
[2] Mendenhall. E. Rethinking Diabetes: Entanglements with Trauma, Poverty and HIV. Cornell University Press 2019
In this episode we catch up with Dr Jonathon Tomlinson, an amazing GP in Hackney. Jonathan fills us in with how he is getting on during the coronavirus crisis. He shares his experience working in a practice in one of the hardest hit areas for coronavirus in the UK (1min 40). He tells me how his team has acted quickly to manage the acute situation but also continues to support the long term conditions for many of his patients in the community.
We talk about some of the many changes in primary care over the last few weeks (5min 40s). These include; phone and video consultations; losing the GP waiting room; sharing clinical decisions and talking more with colleagues. We discuss the effects of coronavirus on those people living in deprivation (10mins 10s) and Jonathon shares some experiences from his practice and his patients (11mins). Jonathan talks about the social determinants of health and the importance of prevention along with all the stuff we are seeing in the media at the moment like PPE (14mins 50s) .
One of the things that GPs can do is advocacy and Jonathon was keen to discuss the work of Dr Rudolf Virchow 1821-1902 (19mins). Virchow is famous for saying that politics is nothing but medicine on a large scale and that our role as doctors is to show the link between social conditions and medical diseases (21mins). Jonathan explains why Virchow’s message is particularly relevant at the moment. We explore the role of a GP in advocacy and coordination of a response to support those who are most in need and vulnerable. We discuss how much our job in primary care should include advocacy on behalf of our patients (26mins) and Jonathon offers some ideas for some steps clinicians can take forward to achieve this. Jonathon mentions collaboration, networks (e.g. The Deep End Network), treating long term conditions. We finish our conversation talking about the importance of caring for our patients (28m 55s), Jonathon shares his favourite book (32m 10s), and he tells us what his magic genie wish would be (34m 40s).
We came dangerously close to touching one-another when we came through the door into my consulting room. I held it open for her so she would not have to touch the handle. She held it open with her left foot just as I let go with my outstretched right hand. I had placed our chairs three meters apart, and we sat down facing one another. I sat with my back to the window which meant that her face was lit by the sun while mine was masked by the shade. It wasn’t a deliberate ploy to expose and conceal, but we noticed it as soon as we looked up at one another. I apologised as she winced in the light and I moved my chair around 90 degrees. Fortunately my room is big enough but I’ve consulted in rooms where social distancing is impossible. Everything felt awkward. Consulting has barely changed in hundreds of years. Illustrations of doctors and patients show them sat down at a distance of two to three feet from one another, sat across a desk, or besides a bed. We barely have to leave our seats to inspect our patients. A stethoscope is the perfect length to stretch across the arms-length divide between us. We can inspect hands for signs of disease or reach over to hold them in comfort or pass a tissue to catch the tears. I have spent the last 20 years working at this distance, learning how to judge how much touch is appropriate, and how to ‘harvest the richness of multisensory exposure’ in order to unpack ‘heartaches’, ‘headaches’, ‘bellyaches’ and more.
I am working in uncharted territories without a map. There are technical guides in abundance, but nothing about the relational aspects of consultations where we are separated by physical distance and fear of contagion.
Henri Cartier-Bresson favoured a 50mm lens for his photography because it was the closest to the natural field of view of a human eye. At three meters distance this takes in a full seated figure from head to toe. At two to three feet apart, the way we used to consult, this field of view takes in only a face.
Seated three meters apart we were both aware of how our bodies were exposed to one-another and we wriggled around trying to find a comfortable position. It felt more like a film set than a clinical consultation. There was no desk or computer screen between us. My PPE: mask, gloves, goggles and apron make me feel ridiculous. I peeled off my gloves and apron and I was about to take off my mask, but the sink in which I needed to wash my hands was just behind my patient. We circled each other awkwardly like cowardly boxers in a ring, before taking turns to wash our hands. We sat down again and looked at each-other once more before removing our masks. I took mine off quickly, snapping the straps sharply while she struggled to tear the straps and ended up slipping it down around her neck.
We wanted to go back to the old ways.
Video
I gazed at myself on the computer screen. I moved backwards and forwards, turned my head slightly left and right, lifted my chin up a little, down a little, moved the webcam left and right. I moved the curtains behind me to one side and a picture on the wall across a few centimetres. I turned the lights down and opened the curtains to let in just the right amount of natural light. In the old days I could finish a surgery and then catch sight of some extravagant nostril hairs, a fuzzball of hair that had been blow-dried on the cycle-ride to work, or a stain on my shirt that a dozen or more patients had stared at all morning. These days I’m seeing what they’re seeing, And the critical self-regard is relentless.
My patients have refused a home visit when they were seriously sick because they hadn’t showered or tidied their flat. They want time to prepare themselves before the doctor lays his judgemental eyes upon them. The clinical gaze is full of moral judgement whether it is intended or not. Look too good and the doctor might not take your symptoms seriously enough, look too bad and they might look disgusted. This Goldilocks zone can be precariously small if you’ve been made to feel you got it wrong before. Using the video consultation software lets us see ourselves as others see us and if we don’t like what we see, we imagine they think the same.
Suddenly my patient appears on the screen besides me. I look at her and smile, but catch sight of my face … and my eyes are focused …. where exactly? If I look at her then I am gazing off to the left, if I look at the camera then it looks as if I am looking at her, but I’m not. If I look at myself (I can’t help it) then I’m looking somewhere else. The concentration required is unnatural and exhausting. She was sitting cross-legged on the floor with the phone placed in front of her. She wants to show me where it hurts and it is easier to do that this way. Yesterday someone wanted to show me a rash on their abdomen and they thrust their phone right up against it. It felt like they had grabbed me by the scruff of the neck and held my face inches away from their waist. I physically recoiled from the monitor, but the image stayed the same, wobbling around, in and out of focus.
She clutched her abdomen to show me where it hurt, could it be her liver she wanted to know, I wanted to answer the same way – by pointing to my own body, but my carefully curated head-shot meant I couldn’t get enough of my body in the field of view. She cocked her head trying to see what I was trying to show her as I fiddled with the camera and stood back and up on the tips of my toes and eventually climbed on my chair. In the old days it was much easier to show (and feel) where it hurt.
“Show me where it hurts”
I have felt uncomfortable asking patients to reveal their bodies on a video link. In the old days, patients could undress behind a screen and I would wait until they were ready, or I would lift their vest to feel their abdomen, or guide the patient into the correct position to examine an intimate part of their body. When I visited patients at home people knew that the doctor was there, and you weren’t afraid that someone might burst into the room. I am sure that the awkwardness of examining bodies by video is felt by doctors and patients.
We are amateurs – like clumsy teenage lovers trying to work out where to start. The technology wasn’t made for this; we weren’t made for this. I am a fan of professional Youtubers Contrapoints and Philosophy Tube and have watched them progress from badly lit monologues into set pieces of performance art. In the old days I liked to imagine good consultations like performance art with my consulting room as the backdrop to a drama performed by patient and doctor improvising with one another. Now I have been evicted from my room to make space for a Hot Hub to see patients with suspected Covid-19 and I am working in a minor surgery suite with a telephone and a webcam perched on top of my computer screen. I see only two or 3 patients a day, one by video, one in my new room and one home visit. My normal complex patients with chronic pain, chronic fatigue, chronic anxiety and complex trauma have largely disappeared from my appointment lists, but I have been calling them to see how they are. Paul Dieppe and Julian Tudor Hart wrote a paper in 1996 called Caring Effects showing how continuing interest and ‘caring about’ as well as ‘caring for’ for patients with chronic pain, reduced symptoms, disability, and analgesic medication use.
For some doctors and some patients I am sure that the new world is a welcome relief from the intensity of physical proximity. In interactions with people who present in existential distress/chronic pain most of the effort clinicians undertake is NOT to listen, not to get absorbed into this black hole of despair. Multi-sensory exposure at close proximity is the situation in which they want to press the button for the ejection seat, or for the trap door under the seat of the patient. When doctors give out these ‘not wanting to be there’ vibes, patients, who are often highly attuned to rejection, pick up on them acutely and the desire to escape is mutual.
Little is known about patients’ experiences of these new ways of consulting. Doubtless it’s good for some. But others have complained about the costs, especially people with pay as you go phone contracts. It isn’t suited to people without phones, people who don’t speak English, elderly patients, people without a quiet space to talk, people with sensory impairment, people who struggle to make themselves understood, people who don’t feel safe at home, people who like to be greeted by a friendly, familiar face, people who are isolated and need a reason to leave their homes.
In a face to face consultation spaces between doctor and patient are tacitly negotiated. Access to bodies by way of a physical examination; access to biology with scans and blood tests; and access to life stories; cannot (or at least should not) be taken for granted. Sometimes permission is given explicitly, for example consent to an intimate examination, but usually doctors explore and patients reveal only so far as they feel comfortable. Consent is gradually conceded (or withdrawn) according to how comfortable they feel, which in turn depends on body language – which is lost when we are not together.
A GP surgery and a doctor’s consulting room are physical spaces where secrets are confessed, mortality contemplated, bodies exposed and biographies unearthed. We call this clinical practice, but in many ways it resembles what happens in a church. People go to church or to the GP in order to think, say and do things they do not want to do or cannot do elsewhere. It is about a safe and symbolic space as well as the people in it. I do not think we can do without consulting rooms any more than we can do without churches.
In the old days, I would meet patients in the waiting room, watch them walk towards me and then accompany them to my room. At the end of the consultation I would sometimes walk them back again. Where they waited and how they walked were details that mattered. But nowadays they appear from nowhere and disappear in an instant. In the waiting room I would see other patients, other doctors and nurses and receptionists. I could sense the mood. Walking around the practice I would meet with colleagues and we would talk about patients we were worried about and stuff going on in our own lives. A lot of problems were solved and support given and received in these chance encounters. Now when we come out of our rooms we move as if surrounded by invisible Zorbs. We pass one another with our backs to the wall, holding our breath. We have more formal catch-ups, which is good for some problems but less suited to others. Patients frequently had chance encounters in the waiting room where gossip was shared and friendships rekindled.
Being with and being around people is as important as talking. When my dad died what my mum missed most of all was his presence. He hadn’t spoken much for a couple of years, but she missed his being more than his words. We all miss our patients being around. Many of our receptionists have been in the practice for years and have very fond relationships with our patients: the poppets and the pains in the arse. We’re doing well under the circumstances, but there is an air of sadness. The loading of intimacy with fear fills me with sadness.
Some things we can be sure about. We are novices but we are resourceful and we are learning fast and we will get better. We will be able to offer patients a choice of initial contact- online, by phone or by video or face to face. Many, quite likely most problems can be solved safely and satisfactorily without a face to face consultation. This way patients and clinicians will be free to spend more time with one another when they really need to. It will be especially valuable in hospitals saving patients the trouble of arduous travel, expensive parking and long waits. More clinicians will be able to work flexibly (from home if they want). There will be less waiting and waiting rooms can be requisitioned for social activities – a purpose they served before, even if it was not explicitly acknowledged. But no matter how long this lock-down and fear of contagion continues we will not lose our desire to be with one another.
In 2009 during the H1N1 flu, a public health consultant came to our practice and described a potential situation so utterly catastrophic that we sunk into a collective state of hopelessness and despair for several days. We blocked out any thoughts of pandemics from then on.
Friday 13th I called a consultant foot surgeon about a patient I was worried about. He said that all his clinics had been cancelled until further notice. I asked him what he was going to do. “Play golf!” he replied cheerfully. Now I like to imagine him redeployed to assist nurses in intensive care for 13 hours a day.
That same day I emailed my sons’ cycling club to suggest they called off the session the following day but they replied to say that they were going to carry on, in line with government guidance. Cheltenham festival was still going ahead after all. It was a harbinger of what was to come. That hard choice between following government guidance or doing your own thing. When you’re dealing with large groups of people – 140 kids in a cycle club or 52 employees split across 2 GP surgeries, you need clear guidelines and operating procedures. And where there is usually just one government guideline there are a multitude of feasible alternatives and a consensus can be hard to find.
Saturday 14th Our next-door neighbour told us that a teacher from our son’s school whose son had been staying over with her children and ours a few days before, had been diagnosed with coronavirus. We looked at our snotty children and thought about the number of times we had kissed them in the last 24 hours and realised that it would be impossible to avoid catching it ourselves.
Sunday 15th In the evening after work I felt vaguely unwell with chest tightness, sore glands and a cough. I couldn’t tell if it was psychosomatic. I’m a poor diagnostician when it comes to my own symptoms. A few years before my psychosomatic illness turned out to be an appendix abscess. I called work to say I planned to stay at home for a week. For the sake of my colleagues and my patients it was better to err on the side of caution.
Monday 16th I arranged to stay in touch with my two trainee GPs by phone and video. One called me at lunchtime about a man in his early 60s who worked as a hospital porter. His wife had called because she was worried about him; he was tired, nauseous and couldn’t get out of bed. No cough, no fever, no chest pain, no past medical history, not on any medication, hardly ever gets sick. I suggested that my trainee ask if he, or rather, his wife, would be happy to postpone a visit but have a follow up phone call the following day. When she called back, his wife was in a state of panic – “Come now! He’s going blue!!” The paramedic arrived at the same as my trainee, seconds after he had a cardiac arrest. They tried to resuscitate him with several rounds of CPR but he didn’t survive. My trainee didn’t even have time to put on any protective equipment. We couldn’t prove that he died because of coronavirus but we couldn’t put the possibility out of our minds.
Since then we’ve learned from personal experience and published data, that men in their late 50s and 60s are dying disproportionately and that sudden deterioration at around day 10 of the illness, with an acute worsening of fatigue is an ominous sign. Half my colleagues are men in their 50s. Many of them, because of their experience, are offering to help in the most hazardous places.
Conversations about the end of life
Last week I spend two days calling my most vulnerable patients and their carers to discuss what they would want if they caught Coronavirus and were sick enough to need hospital treatment. Some of them know what it is like to survive a cardiac arrest and ventilation and some of them would be willing to go through it again. If you are relatively well to begin with oxygen therapy might be all you need, but most people understood that the chance of surviving a cardiac arrest bought on by infection with coronavirus in an already frail body would be negligible. “I’ve had my life doc, let them save their ventilators for people younger than me”, said one woman, who is not much older than I am. If I had overwhelming infection and multiple organ failure I wouldn’t want or even expect my colleagues to try to resuscitate me. Not only would my chance of survival with any quality of life be unacceptably low, but the risk of infecting those treating me would be unacceptably high. We are supposed to have the right to refuse any reasonable treatment, but the problem is that CPR is so often performed when it is completely unreasonable, in people whose hearts have stopped because their bodies are too weak for their hearts to keep going. The refusal of CPR is a reminder to professionals whose reflexes are trained to save lives first and think later, that a peaceful death is possible and preferable.
Some of my patients wouldn’t want to go to hospital under any circumstances. We talked about what critical care might involve – oxygen might be enough. Home treatment with oxygen might be an option, but not just yet. For sons and daughters caring for elderly parents, the greatest worry was who would care for their parents if they themselves got sick. I put a note ‘Patient themselves providing care’ on their records to alert anyone that might treat them in an emergency. I promised to help anyone who chose to die at home.
I’ve never experienced so much gratitude as I did in those 2 days of conversations about serious illness and care at the end of life. It helped enormously that we had nearly 20 years of continuity of care before we talked.
Poverty and inequality
We serve a relatively young, deprived, multi-ethnic population in Hoxton in London’s East End. People in their 50s suffer a burden of diseases like heart disease, lung disease, obesity, diabetes and cancer, that people in wealthier areas don’t experience until they are in their 70s. All of these increase their risk of dying from Coronavirus. Lockdown hits them harder too. Childhood poverty is around 40%, twice the average for England and deprivation for older people is more than three times the national average. Many of my patients work as carers, cleaners, on public transport or on checkouts, shop floors, bars, cafes and warehouses.
In the last month we (my family and I) have been fortunate enough to distract and soothe ourselves by baking, gardening and exercising in the forest or in the garden and streaming movies. Life is different for most of my patients.
Isolation and overcrowding
I look after a family with four children between the ages of 3 and 16 and two adults in a two bedroom, 5th floor flat. One of the children is disabled and autistic, one of the adults is addicted to heroin and alcohol. There are countless variations on this theme of overcrowding, disability, mental illness and addiction.
Violence and abuse
Up to 10% of my appointments used to be spent with people suffering anxiety and chronic pain and for many of them it was related to living in fear. A trip to the doctor was an excuse to come to a place of safety and spend time with someone kind and attentive. We didn’t need to (and often couldn’t) talk about what was going on home. I haven’t seen any of these women in weeks. I haven’t had any reports to complete for social services about children at risk. I don’t know if they have safe places to go, or if anyone is looking out for them if they’re not seeing anyone outside the family home.
Digital hardware and data (streaming/ video/ phone-calls/ internet)
At home we’re online all the time. We pay for unlimited wi-fi. But many of my patients are on pay-as you go data contracts and regularly use up their data just waiting for calls to be answered, never mind Netflix. Some cannot use a smartphone or a computer. Some are illiterate. Some of them run up huge debts with multiple phone contracts. Video consultations with your GP are now commonplace, but the more I do, the more I worry about the people we’re not hearing from.
Bulk buying without a car/ money
We are very well served with local shops where I live in Leytonstone and can get all the fresh produce we want. But supermarkets are being stripped bare of essential produce by people whose cars and wallets are big enough, leaving only scraps for people who live one day or one week at a time, who have to walk and carry everything home. They need to get out more frequently, walk the streets and wait in queues.
Access to green spaces
At the weekend I rode my mountain bike in Epping Forest at sundown. It was beautiful and social distancing was easy. My sons played on the grassy flats at the end of our road. We cooked a barbeque in the garden. At work I spoke to a woman with a eight year-old daughter who has ADHD and anxiety. They live on a 8th floor, north facing flat without a balcony. If they want to go out they have to take a lift or walk down a narrow stair case where social distancing is impossible. Victoria Park, the biggest park in Hackney, has been locked shut for weeks because of adults hanging out in crowds. I know parents with young kids who have barely been outside for a month.
Physical distancing
I cycle 9-10km to work every day. It’s easy to keep my distance and stay fit. I have a job that I enjoy, that pays well where I am surrounded by supportive colleagues. We moved rapidly to a mixture of telephone and video consultations and home working, physically isolating ourselves from our patients.
Many of my patients work in jobs that demand travel and human contact –they are carers, cleaners, bus-drivers, shop staff, teachers, nurses, midwives and pharmacists. Most of them depend on public transport to get to work. They are having more far more face to face contact than I am having as a GP and while I have all the PPE I need, many of them have little or none. Analysis of location data from US cities shows that the wealthier you are the sooner you are able to isolate and the more likely you are to be able to work from home.
No social contact may preferable if your main concern is contagion, but it is still a basic human need. My sons haven’t hugged me so much in years. They want physical reassurance and closeness, more than explanations or soothing words. When staff have been unable to come into work because they’ve had symptoms or been in contact with someone who has symptoms (none of us have been tested) they have all been desperate to come back and be around their colleagues. Before Covid-19 many of our must vulnerable patients rarely left home except to see their GP or practice nurse. Being physically present with someone with whom you feel safe and cared for is something too many of us take for granted. Cautiously I’ve allowed some of them back. We sit with our masks on at opposite sides of the room. One woman I look after, who has already spent weeks in intensive care two years ago and is on the high-risk shielding register asked me to come around to have lunch with her. Her son died just a few months ago, “You know me doc, I’m not afraid to die”.
Precarious employment
I have friends who work in hotels, building, catering, and others who are musicians and artists who have all lost their jobs. Many of my patients earned too little to save and are now without work or money. They are dependent on universal-credit and the kindness of strangers. They may have enough to eat but you cannot live on food alone. We don’t know how long this will last or what jobs might be there when it’s over.
Social capital
I can depend on friends and family, most of whom are as fortunate as I am, to help me out – practically, financially and emotionally. Like most of us, in our socially divided country, we are surrounded by networks of people whose circumstances are similar. Often, I am the only professional person my patients know.
Meaning and purpose
Working in the NHS – being lauded on the news and being clapped in the streets every Thursday evening and thanked all day is something I’ll never forget. We’re taking risks, but despite the overused analogies of war, it’s in no way the same as being in an actual war-zone with explosions going off and bullets flying by. We’re not dealing with the bodies of children who have been maimed by landmines and we’re not getting shot at on the way home. What we do have, now more than ever, is a sense of meaning and purpose combined with public outpourings of appreciation.
All of this is on a background of 10 years of austerity in which the welfare state has been stripped back and public health funding has been stripped bare. The NHS has barely recovered from the most shambolic re-disorganisation by Andrew Lansley in 2012, followed by 8 more years of underfunding. We have seen a rise in insecure employment, and a massive distraction with Brexit which has fuelled a breakdown in social cohesion and undermined public trust in politicians and experts at a time when we need them more than ever.
How will we recover?
We have learned that the NHS can change very quickly when driven by clinical leadership and patient needs. Resistance to Lansley’s disastrous market-oriented NHS reforms resulted in a backlash of criticism accusing the NHS of being intrinsically resistant to change and indifferent to patient needs. Now it has been found to be fleet-footed when the people that work there can see that that they are serving patients and not political vanity or private profits. We’ve been allowed to decide for ourselves what’s most important. In general practice we have rapidly taken up telephone and video consultations and we have concentrated our efforts on the interventions we know make the biggest difference – proactive care for our most vulnerable patients, immunisations for children, primary and secondary prevention of cardiovascular disease and better diabetic control. We have stopped the arduous and pointless CQC inspections, GP appraisals and NHS health-checks. We are talking to each other more than ever about patients we’re worried about and getting second and third opinions about complex decisions.
In the last month we have become better connected with community organisations than ever before. Far more of our patients depend on social support than will ever depend on medical care. Long may this develop and continue.
Further reading
To protect population health it will be essential to avoid a further period of austerity and the associated reductions in social security and public service spending. Instead we must build a more sustainable and inclusive economy. British Medical Journal 27/04/2020 https://www.bmj.com/content/369/bmj.m1557
A bioethicist at the heart of the Italian coronavirus crisis asks: why won’t we talk about the trade-offs of the lockdown?
The generals repeated the old lie, “Dulce et decorum est, propatria mori!” Sweet and becoming it is, to die for one’s country
“Hippocrates and Galen, are still renowned for their wise and innovative advice on medical matters. When it came to plague, they offered guidance, rendered in Latin as ‘Cito, Longe, Tarde,’ which translates as ‘Leave quickly, go far away and come back slowly.’ When the Black Death swept over much of Asia, Europe and parts of Africa in the mid-1300s, such advice was about as good as it got.” Bought to Life
Some did stay, out of Christian duty, desire for fame or because they got ‘hazard pay’ from local communities. The idea of a social contract didn’t come around until the 19th century.
At the start of the 20th century the American medical code of ethics stated, “when pestilence prevails it’s the physician’s duty to continue ministering to the sick even in peril of their own lives”
In 1912 the language was strengthened to say there was, “an obligation to continue taking care of people who posed a contagious threat even if you were not being paid to do so.” Ethics Talk podcast
But how far should this duty reasonably extend? Doctors are already dying from Coronavirus infections contracted in the course of caring for infected patients. Many, if not the majority, lack the recommended protective equipment.
Doctors have always placed themselves at risk in the course of their work. In 2003-4 I joined Medecins Sans Frontieres (Doctors without Borders) and I accepted a job in North West Afghanistan knowing that there were risks including death, because of ongoing conflict. While I was there some of my colleagues were assassinated very close to where I was working. Since then I have chosen not to go back to work in conflict zones, but other doctors continue to do so. Doctors’ attitudes to personal risk in the line of duty vary considerably.
At one end of the spectrum are those, like David Nott, the war surgeon, who wrote, “I have travelled the world for 25 years in search of trouble. It is a kind of addiction, a pull I find hard to resist. It stems partly from the desire to use my knowledge as a surgeon to help people who are experiencing the worst that humanity can throw at them, and partly from the thrill of just being in those terrible places, of living in a liminal zone where most people have neither been, nor want to go.” Others are risk averse and under the current circumstances are avoiding all clinical contact while their colleagues continue to work in intensive care units with patients who have coronavirus infections.
I find myself somewhere in the middle of the spectrum. In 2003 I was single and in search of adventure and I felt invincible. In 2020 have young children and I feel more mortal.
We all have reasons for where we might find ourselves on the risk-taking spectrum. One is what motivates us. Not all doctors are primarily motivated to take risks by the desire to save lives or help people less fortunate than themselves. The motivation may be extrinsic rewards like money or fame. Other motivations include intrinsic values like caring, social justice or self-sacrifice which may derive from upbringing, life experiences or religion. Caring can be viewed as a positive motivation; for example, someone bought up in a caring environment with positive experiences of care and caring, for whom caring is an integral part of their identity.
The need to care for others and sacrifice oneself may also come from a need to repair something flawed, damaged or shameful about oneself, to compensate for low self-esteem. Growing up in a relationship with parents who made someone feel inadequate may result in these feelings persisting into adulthood. The adult tries to compensate by self-sacrifice and risk taking. The sense of being flawed or ‘bad’ drives the need to ‘do good’ while the risk-taking is driven by a sense of ‘just deserts’.
There is a strong sense of this when listening to the war surgeon David Nott who places himself not just in high risk, but unnecessarily high-risk situations. Risk for him is both euphoric and addictive. He is the archetype of a heroic doctor, putting the lives of his patients above concerns for his own life. We might hope for him to be our surgeon in a life or death situation, but we might feel differently if we worked with him.
Doctors work in teams; with other doctors, nurses and health professionals as well as admin staff. It’s easier and perhaps more comforting to imagine that the patient is their only, or at least primary concern, particularly in relation to a war surgeon. A GP has to care for individual patients as well as their practice population. We have to support widows who are grieving and be sure that all the children registered are fully immunized. As a senior partner in my practice I am responsible for over 26000 patients and 40 members of staff. The more I sacrifice myself in the services on one person the less I am available for others.
Brain surgeon Henry Marsh is another heroic doctor whose concern for his patients described in his book First Do No Harm runs to commandeering hospital beds and over-riding clinical colleagues and an open contempt for hospital managers whose concern is the smooth running of the hospital. From an individual patient perspective, you’d want him on your side, but if you happened to need a hospital bed for something other than neurosurgery you might feel differently.
Obligations to individuals and populations come into conflict all the time in medical practice and the extent to which our sphere of responsibility diminishes with distance varies considerably between doctors and between individualistic and communitarian cultures. We live in an individualistic culture that valorizes heroes. We are conservative; suspicious of foreigners and socialism having voted for Brexit and 10 years of Tory rule. We are looking for heroes to save us from Coronavirus.
For the last week I have been self-isolating – with what feels like a typical cough and cold. I don’t have breathlessness or a fever. There’s no way of knowing if it is a mild case of coronavirus. Under other circumstances I would be at work. Presenteeism – the phenomenon whereby healthcare professionals come to work in a state of ill-health that they would advise their patients to stay at home, is rife. But this might be Coronavirus. As the pandemic unfolds we might reach a situation where medical professionals are more likely to be infected than their patients. Dr Gordon Caldwell a consultant physician in Oban, has written about what should happen if he requires ventilation because of coronavirus infection.
If I survive to be weaned off the ventilator (1 in 5 chance) it would be at the expense of 1 staff member with severe Covid 19 and 3 others infected, who in turn could infect other staff, patients, and their own family and friends. Until someone can counter this argument with a convincing statistical, not emotional, case, I have stated that I am “Do Not Attempt Cardiopulmonary Resuscitation (DNACPR” and “Do Not Intubate and Ventilate (DNIV)”
Hospitals as well as doctors might soon become the hubs for transmission of coronavirus in the UK if we continue to follow Italy’s lead. The hero who remains on deck after all the passengers and crew have left the sinking ship is not suited to the present epidemic. Our present-day heroes will have to relinquish the helm while they isolate themselves to protect their colleagues and their patients. They will have to trust their colleagues to take over. They will have to show that we can carry on without them.
Michael West – an organizational psychologist who leads on compassionate leadership for the NHS recommends that the priorities should be listening to staff, removing obstacles to safe and effective work, and providing for their basic needs: safety, rest, nourishment and connection. The lesson from this is that during this crisis every single one of us, will at some point have to be a new kind of hero.
Posted onFebruary 23, 2020|Comments Off on Trauma informed care in General Practice
“In the mid 1990s the CDC and Kaiser Permanente discovered an exposure that dramatically increased the risk for 7 out of 10 of the leading causes of death in the United States. In high doses it affects brain development, the immune system, hormonal systems, and even the way our DNA is read and transcribed. Folks who are exposed in very high doses have triple the lifetime risk of heart disease and lung cancer and a 20-year difference in life expectancy. And yet, doctors today are not trained in routine screening or treatment. The exposure I’m talking about is not a pesticide or packaging material it’s childhood trauma”.
Nadine Burke Harris
In this blog, I’d like to suggest what routine screening and treatment might look like in primary care/ general practice. In previous blogs I’ve focused on care for individuals, but here I want to describe a population approach.
Childhood trauma (also called ACEs Adverse Childhood Experiences, is a risk factor for disease, and like other risk factors, for example smoking, the greater the exposure, the greater the risks. Maltreatment that begins earlier in life, is more severe and continues for a longer duration is associated with the worst outcomes. The harm is a result of physiological and behavioural changes; what I have recently described as the ‘Trauma World’ also called ‘Toxic stress’. The word ‘trauma’ is often used to refer to this response, rather than the traumatic events. This is what makes trauma traumatic. For example, PTSD often develops after a supportive partner dies, because their partner provided them with enough resilience to cope with the trauma of their past experiences. Trauma is a legacy of emotional hypersensitivity (or the opposite, alexithymia/ numbness), toxic shame, dissociation and harmful coping strategies. Survivors present to GPs with chronic anxiety, recurrent panic attacks, chronic pain and chronic fatigue. They are more likely to suffer from multiple long-term conditions like diabetes, vascular and lung diseases, autoimmune diseases and cancer at younger ages. As well as being at risk of ill-health they are at risk of violence, abuse, homelessness and destitution. They are less likely to have attended for vaccinations or screening for cancer and they are more likely to smoke, drink alcohol excessively and use drugs including potentially hazardous combinations of prescribed drugs.
A GP practice would want to identify people suffering from trauma in order to diagnose diseases early, to prevent them from developing and to provide appropriate social and psychological support.
A GP practice has a list of registered patients (a denominator) and they will know the numbers of people with long-term conditions such as diabetes, hypertension and depression (the numerators), and they will be invited in for regular reviews. It is easy to identify these people because they have a diagnosis. Because ‘trauma’ is not a diagnosis, it is not tested for or documented like other long-term-conditions so we do not yet have a reliable way of identifying patients who have been affected. A recent study found that trying to identify patients by searching their records for evidence of Adverse Childhood Experiences found only about 1% of those they expected to find.
There is a code for ‘History of complex trauma in childhood’ which has only recently been introduced, but despite my interest in the subject, I am yet to use it because I’m not sure that many people would want it in their medical records. They might rightly fear that other clinicians would bring it up uninvited or worry that whatever symptom they sought help for would be blamed on ‘trauma’. A history of trauma may be hidden in the text of a consultation or a hospital letter, but we cannot search the electronic records in this much detail as we can for diagnostic or problem titles. In any case, it is the presence of trauma, rather than a history of adversity that we are trying to identify. So instead of searching for a diagnosis we could include people with symptoms that are suggestive, if not diagnostic of a past history of trauma; problems like chronic anxiety, chronic pain, irritable bowel syndrome, chronic depression, OCD, self-harm, personality disorders, alcoholism, opiate/ benzodiazepine addiction – and I would include anyone on long-term anti-depressant or antipsychotic medication, regular opiate or benzodiazepine prescriptions.
Patients identified this way might represent 10-50% of a GP practice population depending on issues like deprivation and immigration. Having identified patients, they should be invited in for an initial review and if suitable (more on ‘suitability’ below) added to an ‘at risk’ register for continued annual reviews. Many of these patients will be known to be suffering trauma, and some will not. At the initial review both doctor and patient need to agree whether a regular review would be useful. If there is a disagreement, then the patient’s preference is what matters, after all it’s for their benefit. I would caution against assuming that non-attendance is a sign of disagreement, since people whose lives are insecure and full of anxiety often struggle to attend appointments
The review:
Comprehensive
An annual review should be comprehensive so that all the patient’s long-term conditions are reviewed at the same time, so as not to overburden them with appointments. Their lives are usually filled with bureaucracy as it is. I would include:
A co-created problem list.
It’s been enormously helpful for me to look at patient’s records with them and agree on what to call their different conditions and which are active and significant. It’s an opportunity to think about what the prefix ‘chronic’ means when applied to pain, anxiety or depression. I quite often discover that embarrassing problems like incontinence, mentioned years ago have not been bought up since and are not ‘minor, past problems’ but are definitely ‘significant and active’. In my experience, the process of agreeing on this list together helps both patient and clinician to join-the-dots and see how different conditions relate to one another. At this point it is not unusual for childhood trauma to be bought up and discussed in detail or at least acknowledged. This is a good opportunity to explain the purpose of the review.
An important point here is to recognise that significant childhood trauma is a risk factor for a wide range of diseases and the point of the review is to treat them early or prevent them so far as possible. This can help to reassure patients that far from attributing all their symptoms to trauma, we are staying vigilant for the biological consequences of a lifetime of stress in a way that is safe, structured and planned.
Disease identification and prevention
For many people the experience of past trauma leaves them in a state of tension and hyperarousal, so assessing for hypertension, cardiovascular disease and inflammatory diseases such as arthritis and colitis should be included. Screening for cancer, vaccinations for HPV, childhood viruses, hepatitis and flu, sexual and reproductive health are all especially relevant for people with a history of trauma who may, as a result of insecure, chaotic lives have missed out. Because trauma increases the risks of developing disease, they have more to gain from screening than people more fortunate.
Risk factors relating to coping
People who have experienced significant past trauma often resort to coping strategies that in themselves can be harmful: smoking, excessive drinking, illicit drug use, eating disorders, unsafe sex and so on. We should ask about coping strategies and offer support with smoking cessation and alcohol services, sexual and reproductive health and whatever else is required. We should help them find other, less harmful ways of coping.
Social security
One of the most traumatic events that effects my patients who have already experienced trauma is having their benefits stopped after assessment by DWP. Over 90% of them succeed on appeal but have nothing to live on for 6 months or so while waiting for the process. We need benefits advisers to be available to help people when they need it, within GP surgeries. Social security also includes personal safety and many women that I look after with a history of childhood trauma also have ongoing trauma from domestic violence, so we should ask about this – the HARK questionnaire is a useful aid. We can then refer to specialist supportive services. Young people are at risk of gang violence and exploitation and should be offered support.
Mental health
Many patients will already be suffering from diagnosed mental illnesses, but others will have undiagnosed problems like anxiety, panic disorder, OCD and autistic spectrum disorders. Including mental health as part of a general healthcare review helps to create a culture in which a healthy mind and body are considered together.
Medication review
People with a history of significant trauma are often prescribed a lot of drugs to help alleviate their symptoms and treat their various long-term conditions. A medication review is an opportunity to talk about which drugs are helping and which ones are no longer useful and which ones are harmful; to check for side-effects, interactions and risks including dependence and accidental overdose. We have a clinical pharmacist in our practice who can help with medication reviews including tapering regimes for people who want to come off harmful drugs.
Social prescribing and social isolation
One of the consequences of trauma is that survivors are more likely than others to be isolated and lonely. Annual reviews could take the form of ‘group consultations’ already being used successfully for diabetic annual reviews. There could be a social space in the practice, in the waiting room if it is big enough, where people can get a cup of tea and sit around tables where they can chat while waiting to see a clinician. Some people much prefer to be in their own space, so they need to be made to feel safe and comfortable as well. Most practices can refer patients to social prescribing to help patients find safe places to be doing things with other people in the community.
Physical wellbeing
Bottom up therapies are things that you can do to feel more in control of your body. It can be anything from knitting to yoga, from gardening to parkrun. Nerve fibres from the body travel up to the brain, so that things that make our bodies feel capable, controlled and strong also help our minds to feel the same way. For many people this is much more effective (and acceptable) than psychological therapies. Most practices can refer for exercise programmes and some are even introducing other activities like tai chi and therapeutic gardening.
Nutrition
It is hard to be feel well if you are unable to afford to eat well, if your diet is unhealthy or food is associated with shame. Programmes like Food For Life run by Shoreditch trust can help people learn to change their relationship with food https://www.shoreditchtrust.org.uk/health-and-wellbeing/food-for-life/.
Conclusions
This is an idea and not something that I have implemented, yet. From a GP perspective it might seem like a lot of additional work, but I suspect that most people identified will already be coming in for a review because they have previously been diagnosed with other long-term conditions. It will identify new patients by including a new set of long-term conditions like chronic pain and addiction. I hope that it upsets the Bio-psycho-social hierarchy by making social security, mental health and physical health equally important. I hope too, that it helps to reduce the risks of diagnostic overshadowing by taking a proactive approach to the early identification of disease in people at high risk. Most of all I hope that it helps doctors and patients to come to a better shared understanding of one another by co-creating a problem list and thinking about why it looks that way and what the implications are. And from this I hope to shine a light on hope and salutogenesis.
John sat next to his mum, an elderly, anxious looking woman who did most of the talking. He rubbed his palms hard together, as if trying to rub out a stain while she talked. He was sweating and his right leg kept trembling. He clamped his hands between his thighs to keep his leg and hands still. Mostly he looked down, without focusing, at the floor in front of him. He wore a black jacket over a grey tracksuit with white trainers that had seen better days. He was new to the practice, though I had met his mum a few times before. He wasn’t long out of prison and Janet, his mum, had told me a while ago that she wanted to bring him to see me when he got out. Fortunately the recent spell inside had been short and we had a pretty decent set of notes from his previous GP.
Before he came in I looked at his ‘problem’ list. The electronic patient (medical) record (EMR) has a list of Active and Past Problems, sub-categorised into Significant and Minor. A patient’s problem becomes a Problem in the EMR when it is picked up by the EMR and ascribed a code. A Problem can be a diagnosis, a symptom, or anything else a patient reports that a doctor or a medical summariser adds to the record, so long as it is picked up by the EMR (it comes up in blue text as you type it in). Problem codes aren’t (though I would like them to be) a definitive list of a patient’s problems, but they can be useful. John’s problem list ran to about 160 entries over 4 pages. There were Problems that weren’t problems like, ‘Telephone call to patient’ and ‘results discussed’ as well as Past Problems that I suspected should have been Active Problems like, ‘Anxiety’ and ‘Depression’. Some Minor Problems like ‘Alcohol Problem Drinking’ and ‘Overdose of opiates’ I thought were probably Significant. Problem lists accrue over years and if they are not ‘tidied up’ it becomes impossible to see what problems are ‘Active and Significant’ because they are mixed up with everything else. Another issue is that different problem codes are used to refer to the same problem, for example:
Anxiety states (Significant Past)
O/E anxious (Minor Past)
Generalised Anxiety Disorder (Significant Past)
Anxiety NOS (Minor Past)
Anxiety with depression (Significant Active)
Panic attack (Significant Past)
Agoraphobia (Minor Past)
Social Anxiety (Minor Past)
Irritability and anger (Minor Past)
Often the same Problem code is there repeatedly; there were 5 Anxiety States, 4 O/E anxious and 3 Anxiety NOS. as if anxiety is something new each time, rather than a chronic, enduring state.
Problems relating to anxiety were a feature of his problem list from the age of 11 up to his present 41 years.
Other Problems referred to physical symptoms and conditions that frequently accompany anxiety:
Dyspepsia (8 times, Significant Past, 3 times, Minor Past)
Bloating symptom (5 times, Minor Past)
Abdominal pain (5 times, Minor Past)
Chest pain (4 times, Significant Past
Dizziness
Feels Faint
Insomnia
Urinary symptoms (3 times, Minor Past)
Burning symptom
Going through a problem list is like examining a crime scene for evidence in order to make sense of what has gone on. A problem list is limited by culture, assumptions, omissions, misunderstandings and mistakes. It serves as a tool for audit and finance – we need to know how many patients we have with depression/ diabetes/ cancer/ heart disease and so on so that we know can make sure that we call them in at regular intervals for proactive, preventive care and get paid for it. Because of this, certain problems like these are more reliably coded than others. The presence of multiple problem codes referring to anxiety over a lifetime suggest that anxiety isn’t just situational, but has something to do with what happened in childhood or perhaps a genetic/ familial trait. Taken in conjunction with multiple related physical symptoms, the issue looks more like a lifetime of hyper-arousal – a state of chronic fight of flight than of anxiety alone.
One consequence of being stuck in a state of ‘fight of flight’ is exhaustion. This hyper-vigilance is unsustainable. In childhood it comes across as hyperactivity or ADHD, but with increasing age this gives way to exhaustion with chronic fatigue, depression and chronic pain, or cycles that swing from mania or hyperactivity to depression and numbness. I note that John has ‘Emotionally Unstable Personality disorder [replaced Bipolar disorder]’ among his Active Significant Problems. For some people, this chronic stress causes autoimmune diseases like inflammatory bowel disease, connective-tissue disease or inflammatory arthritis.
There were Problems relating to pain:
Abdominal Pain
Generalised pain
Back pain
Low Back Pain
Chronic Low Back Pain
Lumbar Disc Degeneration
Sciatica
Pain in leg
Radiculopathy NOS
Neck pain
Cervicalgia
I looked for Problems that suggested ways of trying to cope with chronic anxiety, depression, exhaustion and pain.
Opiate misuse
Diazepam dependence
Alcohol problem drinking
Self harm
Accidental overdose
Suicide attempt
The problems suggested something that Daniela Seiff wrote about in Understanding and Healing Emotional Trauma called The Trauma World. I’ve adapted it to use in practice – as shown in the slide below. The Fight or Flight response which may include psychological symptoms of anxiety and hyperactivity as well as physical symptoms like irritable bowel syndrome and palpitations comes under hyper-arousal. These are usually the most obvious or visible symptoms. The flip-side, the ‘freeze or flop response’ includes fatigue, alexithymia (numbness) and chronic pain and comes under hypo-arousal. Toxic Shame refers to pervasive self-blame and may include suicidal behaviour and self-neglect. Symptoms like depersonalisation, derealisation, and functional neurological symptoms like non-epileptic seizures are examples of Dissociation. The use of stimulant or sedative drugs – prescribed or illicit, comes under ‘Coping’. According to this model, addiction is a symptom of The Trauma World, not something separate, or even the primary problem. In red I have written words that refer to the experiences that people who live with The Trauma World suffered when their trauma was committed and frequently continue to suffer in their interactions with medical (and other) professionals; cruelty, disbelief, blame and rejection/ chaos.
There are no simple answers to Trauma World, but there is a mirror image that I have found to be useful, which I call The Healing World.
Where there has been cruelty we can be kind, where there has been disbelief, validation, where there has been blame and shame, vindication and where there has been chaos (and rejection) commitment and consistency, demonstrated by continuity of care. The fingers and thumb don’t mirror the Trauma World, but do serve as a guide for what’s needed. Mind refers to feelings, memories and thoughts which can be helped by therapy. Body refers to physical activity which might be yoga, Tai Chi or knitting, singing, dancing or baking. Something where the focus of attention is on doing things controlled and creative and ideally rhythmical with the body. Biology refers to everything that goes in the body – food and drink, even fresh air. It is a reminder that medicines are only a small part of The Healing World and that what you put in your body affects every part of your body. Positive human relationships have been proven to be the most important factor in recovery from trauma. People are often isolated, lonely and frightened of human interaction, afraid of what other people might think of them or say about them. Feelings of shame, anxiety and depression colour interactions with pessimistic expectations; ambiguous social cues are interpreted negatively. This can be so hard to overcome, and may take years and long-term relationships and unconditional love. A friend and survivor of trauma who runs groups for men who were abused reminds me that, “there are too many of us for you [GPs] but you can help us to help ourselves by providing space for us to meet and run peer support groups'”
Social security is absolutely vital. It is why there is The Trauma World has a social gradient; people who are deprived have fewer resources to buffer the effects of trauma and may live with the threats of violence and destitution. Social security wraps around everything else; make a fist and your thumb wraps around your fingers.
With John beside me, we look at his problem list together. One significant and profoundly useful act, is to agree about what Problems are Active and Significant and what labels accurately describe his symptoms. There no Problem codes for “The Trauma World’ or ‘Complex Trauma’ or even ‘Complex PTSD’. There is ‘Other PTSD’ and ‘Chronic Anxiety’, ‘Chronic Depression’ and ‘Chronic Pain’. We add ‘Irritable Bowel Syndrome’ and ‘Irritable Bladder’. After ‘Other PTSD’ I add a note – ‘discussed with patient, see consult 20.01.2020’ If patients are to receive the benefits to which they are entitled, then at the very least they need a medical report that is accurate and has a list of mental health conditions – in John’s case, Generalised Anxiety Disorder, Panic Disorder, Agoraphobia, Complex PTSD, Depression, History of Self Harm and Suicide Attempts. Emotionally Unstable Personalty Disorder may be unacceptably pejorative, but it’s might be of use in a benefits claim.
I don’t know what happened when John was growing up. I’m not at all sure that it’s necessary for me to know. Probably only if and when John wants to bring it up. There’s enough in his Problem list to know that ‘stuff happened’. Usually though, once we’ve worked through the list and seen the pattern, we’ve laid down a foundation for trust and the past comes out. In that case I document it and leave a reference next to the problem title, so that in future another doctor can look it up without John having to go through it all again.
The Trauma World and the Healing World are grounded in patient experiences and clinical practice. They are a call to action. They demand that we take notice of the bigger picture, that we stop making distinctions between mind and body, that we pay attention to shame and injustice and do something to make a difference.
London Health Emergency
Founded in the autumn of 1983, London Health Emergency is the country’s biggest and longest-running pressure group in defence of the NHS.